Download
1 / 41
640 likes | 1.28k Views
Antineoplastic drugs. Dr. Elayan, 2015. Cancer a disease of cells characterized by the shift in the control mechanism that govern cell proliferation and differentiation. Special Characteristics of Cancer Cells •Uncontrolled Proliferation •Dedifferentiation and loss of function

E N D
Antineoplastic drugs Dr. Elayan, 2015.
Cancer a disease of cells characterized by the shift in the control mechanism that govern cell proliferation and differentiation. Special Characteristics of Cancer Cells •Uncontrolled Proliferation •Dedifferentiation and loss of function •Invasiveness (Spreading) •Metastasis (spread of cancer from its primary site to other places in the body
Management of Cancer Surgical Radiation Chemotherapy If cancer has not spread, the best option is surgery and cure. skin cancers, cancers of the lung, breast, and colon. If the tumor has spread to local lymph nodes only, these can also be removed. • If surgery cannot remove all of the cancer, the options for treatment include radiation, chemotherapy, or both. Some cancers require a combination of surgery, radiation, and chemotherapy.
Chemotherapy • It is the treatment of disease by chemicals especially by killing micro-organisms or cancerous cells. • In popular usage, it refers to antineoplastic drugs used to treat cancer or the combination of these drugs into a regimen.
Types of Therapies: • Adjuvant: Additional treatment after the primary treatment to lower the risk that the cancer will come back. • Neo-Adjuvant therapy : Treatment as a first step to shrink a tumor before the main treatment. • Concurrent therapy: When two or more therapies are given together, such as chemotherapy and radiation.
Cell Cycle • G0 : A resting phase. • G1 : Cells increase in size. • S : DNA replication occurs. • G2 : Gap between DNA synthesis and mitosis, the cell will continue to grow. • M : Cell growth stops ,and cellular energy is focused on division into two daughter cells.
Principles of cancer chemotherapy • Goal of treatment: • • The ultimate goal of chemotherapy is cure. i.e. long term disease free survival. • • If cure is not attainable, then the goal becomes palliation i.e. alleviation of symptoms and avoidance of life-threatening toxicity. • • The neoplastic cell burden is initially reduced either by surgery and /or radiation followed by chemotherapy or combination therapy.
Principles of cancer chemotherapy, con... 2. Indications for treatment: • Chemotherapy is indicated when neoplasms are disseminated (Spread over a large area)and are not cured by surgery. • Chemotherapy is also used as a supplemental treatment to attack micro metastasis following surgery and radiation treatment.
Principles of cancer chemotherapy con… 3. Tumor susceptibility and growth cycle: • Rapidly dividing cells are generally more sensitive to anti cancer drugs. The fraction of tumor cells that are in replicative stage of their cycle are most susceptible. • Non proliferating cells (those are in Go phase) usually survive the toxic effects of many of these agents.
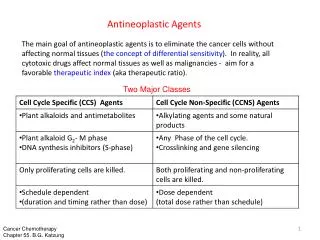
Principles of cancer chemotherapy con.. 4. Cell cycle specificity of drugs: • The normal and tumor cells differ in the number of cells that are in various stages of the cycle. • Chemotherapeutic agents that are effective only against replicating cells are called cell cycle specific (CCS) drugs. • Others are said to be cellcycle non specific (CCNS) drugs. • The non specific drugs have more toxicity in cycling cells and are useful against tumors that have low percentage of replicating cells.
Principles of cancer chemotherapy con.. • CCS – effective against hematological malignancies and in solid tumors with large growth fraction. • CCNS drugs – solid tumors with low growth fraction solid tumors • CCS drugs are given after a course of CCNS • 5. Tumor growth rate: • • The growth rate of most solid tumors is initially rapid, but decreases as tumor size increases, because of unavailability of nutrients and oxygen. • Reducing the tumor burden through surgery or radiation promotes the remaining cells growth into active proliferation and increases their susceptibility to chemotherapeutic agents.
Principles of cancer chemotherapy con.. 6. Treatment regimens and scheduling: •Drugs are administered on the bases of body surface area. •Destruction of cancer cell follows first order kinetics , i.e. a given dose destroys constant fraction of cells. (Log kill) Visible tumor = 1g or 10⁹cells. Each cycle of therapy kills less than 99% of the cells, so multiple cycles are necessary to kill all tumor cells. Magnitude of a tumor cell kill is a logarithmic function: 4 log kill means reduction from 10¹² to 10⁸
Log kill if treatment leads to a 99.999-percent kill, then 0.001 percent of cells would remain. This is defined as a five-log kill . At this point, the patient will become asymptomatic, and the patient is in remission For most bacterial infections, a five-log (100,000-fold) reduction in the number of microorganisms results in a cure, because the immune system can destroy the rest. However, tumor cells are not as readily eliminated, and additional treatment is required to totally eradicate the leukemic cell population. Combine drug therapy is more successful than single drug treatment. •In combine therapy the drugs must have different toxicities & different mechanisms of action.
Principles of cancer chemotherapy con… Effects of various treatments on the cancer cell burden:
Clinical Considerations 1. Early intensive start to the treatment is helpful 2. Complete remission is the goal of chemotherapy 3. Combined chemotherapy is useful - Drug regimens or effective designing of number of cycles can reduce large tumour burden and delayed emergence of resistance 4. Combined chemotherapy can be curative when applied to minute residual tumour cell population after surgery or radiation 5. Treatment must continue past the time when cancer cells can be detected using conventional techniques
Toxicities Bone marrow depression – limits treatment Buccal mucosa erosion – due to high epithelial turnover (stomatitis, bleeding gums) GIT: Diarrhea, shedding of mucosa, hemorrhage Nausea, vomiting – CTZ direct stimulation Skin: alopecia Gonads: oligospermia, impotence, amenorrhea and infertility Lymphoreticular system: Lymphocytopenia and inhibition of lymphocyte function – loss of host defense mechanism – susceptibility to infections Carcinogenicity Teratogenicity and Hyperuricemia
Alkylating Agents Nitrogen Mustards • Mechlorethamine • Cyclophosphamide • Ifosfamide Nitrosoureas • Carmustine • Lomustine Alkyl sulfonate • Busulfan Platinum complexes • Cisplatin • Carboplatin
- Nitrogen mustards inhibit cell reproduction by binding irreversibly with the nucleic acids (DNA) - After alkylation, DNA is unable to replicate and therefore can no longer synthesize proteins and other essential cell metabolites - Consequently, cell reproduction is inhibited and the cell eventually dies from the inability to maintain its metabolic functions. Alkylating Agents Mechanism of Action:
Nitrogen Mustards Mechlorethamine: (MUSTARGEN) Unstable, given IV immediately after being made up Part of MOPP (Mechlorethamine – oncovine-prednisolone and procarbazine) in Hodgekin`s lymphoma . Toxicity: Severe Vomiting bone marrow toxicity (myelo and immunosuppression) tissue damage with extravasation
Ifosphamide longer half life & greater activity than cyclophosphamide Given IV with MESNA (2-mercaptoethane sulfonate). Converted by liver cytochrome P450 to active & toxic metabolites. Toxicity: N&V, neurotoxicity (confusion), nephrotoxicity, hemorrhagic cystitis or hematuria (prevented by concurrent MESNA), cardiac toxicity with high dose, bone marrow toxicity used mainly in testicular tumor
Alkylating agents Nitrosoureas Inhibits DNA, RNA and protein synthesis lipid soluble (cross blood-brain barrier) Carmustine (BCNU) : IV infusion over 1-2hrs Lomustine (CCNU) : taken orally Effective against brain tumors and also in Hodgkin's lymphoma Toxicity: profound delayed and cumulative bone marrow depression, N&V, pulmonary fibrosis (6 months after therapy to 15 years after), renal damage, reversible liver damage and leukemia.
Alkylating agents Alkyl sulfonates Busulfan Well absorbed orally; plasma half-life 2-3hrs Active against Chronic Myeloid Leukemia Toxicity: N&V, bone marrow depression (stem cells), pulmonary infiltrates and fibrosis.
Platinum complexes Cisplatin Cisplatin is the cornerstone drug in the modern management of head and neck cancer Mechanism: Covalent crosslinks with GG base pairs (bends DNA)
Platinum complexes: Cisplatin Pharmacology: IV, not effective orally; most (90%) bound to plasma proteins. concentrates in liver, kidney, intestine and ovary; excreted in urine. Toxicity: N&V, diarrhea, hypersensitivity reactions (rashes), renal damage (reduced with hydration), ototoxicity with high frequency hearing loss and tinnitus, peripheral sensory neuropathy (paresthesia and loss of proprioception), bone marrow depression.
Antimetabolites Structurally related to normal compounds that exist within the cell. Folate antagonist: Methotrexate (Mtx). Purine antagonist: 6-Mercaptopurine (6-MP) Azathioprine. Pyrimidine antagonist: 5-Fluorouracil (5-FU) Effects are in S-phase (cell-cycle specific).
Folate antagonist: Methotrexate Mechanism of action: Folic acid is an essential dietary factor. It is converted to tetrahydrofolate cofactors essential for the synthesis of precursors of DNA(thymidylate and purines) and RNA (purines). Methotrexate inhibits the enzyme dihydrofolate reductase (DHFR) causing partial depletion of the tetrahydrofolate cofactors required for synthesis of thymidylate and purines. In addition, methotrexate is converted to a series of polyglutamates (MTX-PGs) in both normal and tumor cells and inhibits the thymidylate synthase (TS).
MethotrexateCont.. Therapeutic uses: MTX is effective against acute lymphocytic leukemia, Choriocarcinoma (Choriocarcinoma of the placenta during pregnancy) Burkitt lymphoma in children (a type of non-Hodgkin's lymphoma) breast cancer head and neck carcinomas. low-dose MTX is effective against certain inflammatory diseases, such as severe psoriasis,rheumatoid arthritis and Crohn disease.
Routes of administration: Oral, IM, IV, intrathecal. MTX may cause crystalluria . Adverse effects: MTX causes stomatitis, myelosuppression, erythematic, rash, urticaria, and alopecia. • Most frequent toxicities: N, vomiting, and diarrhea. • Adverse effects can reversed by leucovorin. Long-term use of MTX may lead to liver cirrhosis. Neurologic toxicities: subacute meningeal irritation, stiff neck, headache, and fever. Rarely, seizures, encephalopathy or paraplegia. • Contraindications: pregnancy. alopecia.
Purine antagonist: 6-Mercaptopurine Mechanism of action: 6-MP inhibit the conversion of inosine monophosphate to adenine and guanine nucleotides that are building blocks for RNA and DNA. 6-MP converted to 6-MPribose phosphate (6-thioinosinic acid, or TIMP) TIMP inhibits the first step of de novo purine-ring biosynthesis. TIMP is converted to thioguanine monophosphate (TGMP), which can be incorporated into RNA. The deoxy-ribonucleotide analogs that are also formed are incorporated into DNA. This results in nonfunctional RNA and DNA.
Purine antagonist: 6-Mercaptopurine Pharmacokinetics: Oral administration, well distributed except for the cerebrospinal fluid. Metabolized in the liver. The parent drug and its metabolites are excreted by the kidney. Adverse effects: Bone marrow depression is the principal toxicity. Side effects also include anorexia, nausea, vomiting, and diarrhea. Hepatotoxicity in the form of jaundice has been reported in about one third of adult patients.
Pyrimidine antagonist: 5-Fluorouracil (5-FU). Mechanism: Converted in to 5-fluoro- 2deoxyuridine monophosphate (5-FdUMP),which inhibits thymidylate synthaseand blocks the conversion of deoxyuridilic acid to deoxythymidylic acid. 5-FU incorporated into RNA, interferes with RNA synthesis and causing cytotoxic effect. 5-FU produces its effect in the S phase of the cell cycle.
Uses: Pyrimidine antagonist: 5-Fluorouracil Treatment of slowly growing solid tumors (colorectal, breast, ovarian, pancreatic, and gastric carcinomas). Leucovorin (Folinic acid ) enhances the effect of 5-FU by inhibiting thymidylate synthase. Folinic acid is used in combination with 5-FU in treating colon cancer. Pharmacokinetics: Because of its severe toxicity to the GI tract, 5-FU is given IV or, in the case of skin cancer, topically. Adverse effects: Nausea, vomiting, diarrhea, and alopecia, severe ulceration of the oral and GI mucosa, bone marrow depression. 5-FU causes “hand-foot syndrome” is seen after extended infusions (reddening, swelling, numbness and skin peeling on palms of the hands and the feet)
Antineoplastic Antibiotics:Doxorubicin Mechanism of action: Blocks synthesis of DNA and RNA; DNA strands scission – by affecting topoisomerase II. Free oxygen radical generation Clinical uses: Breast carcinoma, Ovarian carcinoma, Testicular carcinoma Thyroid carcinoma, Lung carcinoma Given by rapid IV infusion, distributes widely except to CNS. Toxicity: N&V, severe local tissue damage with extravasation, diarrhea, fever, transient ECG changes, ventricular arrhythmia, cardiotoxicity, anaphylactoid reactions and bone marrow depression.
Microtubule Inhibitors: Vinca alkaloids: Vincristine, Vinblastine. Plant alkaloids now produced synthetically. Mechanism: Antimicrotubule (Mitotic spindle). Binds to tubulin, inhibits tubulin polymerization into microtubules which are a major component of the mitotic spindle. Given by IV infusion to treat various types of leukemia. Vincristine is occasionally used as an immunosuppressant. The main side effects are: peripheral neuropathy, hyponatremia, constipation and hair loss.
Hormonal Agents Glucocorticoids Prednisone Direct antitumor effects are related to their lympholytic properties. Glucocorticoids can inhibit mitosis, RNA synthesis, and protein synthesis in sensitive lymphocytes. Considered cell-cycle nonspecific . Resistance to a given glucocorticoid may develop rapidly and typically extends to other glucocorticoids.
Tamoxifen Mechanism: Competitive inhibitor of estradiol binding the estrogen receptor. Pharmacology: oral; metabolized in liver to active metabolites. Trans 4-hydroxytamoxifen (25-100 more potent than tamoxifen) Therapeutic Use: Estrogen-dependent breast cancer Toxicity: N&V, hot flashes, transient increase in bone or tumor pain when cancer has metastasized
. Aromatase inhibitors (AIs)Exemestane, Letrozole Aramatose is the enzyme that synthesizes estrogen. AIs work by inhibiting the action of the enzyme aramatase which converts androgen into estrogen. AIs are used in the treatment of breast & overran cancers in postmenopausal women. As breast tissue is stimulated by estrogens, decreasing their production suppresses recurrence of the breast tumor tissue.
Tyrosine- kinase inhibitors (TKI) Imatinib & Geftinib Tyrosine kinases are enzymes responsible for the activation of many proteins by signal transduction cascades. Effective anti-tumor agents and anti- leukemic agents.
Tyrosine- kinase inhibitors (TKI) Imatinib used in the treatment of multiple cancers, e.g. Philadelphia chromosome-positive (Ph+) chronic myelogenous leukemia (CML). tyrosine kinase enzymes are turned on and off as needed. In Ph-positive CML cells, one tyrosine kinase enzyme, BCR- Abl, is stuck on the "on" position, and keeps adding phosphate groups causing abnormal cell proliferation. It is present in 95% of patients with (CML). Imatinib blocks this BCR- Abl enzyme, and stops it from adding phosphate groups. As a result, these cells stop growing, and die.
Monoclonal antibodies Trastuzumab, Rituximab, Ibritumomab Directed at specific targets and often have fewer adverse effects. • Designed to recognize and find specific abnormal proteins on cancer cells. • Each monoclonal antibody recognizes one particular protein. Three types of monoclonal A-bodies: Trigger the immune system to attack and kill cancer cells. E.g. Rituximab 2. Stop cancer cells from taking up proteins E.g. Trastuzumab 3. Carry cancer drugs directly to cancer cells These are called conjugated MABs. E.g. Ibritumomab