Download
1 / 31
310 likes | 455 Views
Grant County Health District Measles Outbreak April – July 2008. Dr. Alex Brzezny, HO Peggy Grigg, GCHD Administrator Jackie Dawson, Region 7 Epi. History of Measles. References to measles can be found as far back as the 7th century A.D.

E N D
Grant County Health DistrictMeasles OutbreakApril – July 2008 Dr. Alex Brzezny, HO Peggy Grigg, GCHD Administrator Jackie Dawson, Region 7 Epi
History of Measles • References to measles can be found as far back as the 7th century A.D. • Described by Rhazes (Persian philosopher and physician) in the 10th century A.D. as "more dreaded than smallpox" • Before the 1963 measles vaccine: • Approximately 3 to 4 million cases • Average of 450 deaths a year in the U.S. • Epidemic cycles occurring every 2 to 3 years • >1/2 the population had measles by 6 yo • 90% had measles by 15 yo
Measles Control Goals by WHO Region, 2006 Americas, Europe, E. Mediterranean, W. Pacific have elimination goals 2010 2010 2012 2000 Africa and SE Asia have mortality reduction goals
CDC – Measles Update • Measles outbreaks are ongoing in: • Switzerland • Israel • Europe • Measles is endemic in many countries including: • Japan • India • Serologic and virologic specimens (serum, NP wash/swab & urine)should be obtainedfor measles virus detection and genotyping • Laboratory testing should be conducted in the most expeditious manner possible
CDC Measles Summary • January 1 - April 25, 2008 • 64 confirmed measles cases in 9 states • Highest # for the same time period since 2001 • Outbreaks (3 or more cases linked in time or place) are ongoing in AZ, NY, MI & WI • 10 recent patients acquired measles abroad • Remaining cases linked to imported cases
Measles • Measles is classified as morbillivirus of the family Paramyxoviridae • Virus enters the respiratory tract via droplet nuclei and multiplies in epithelial cells • Incubation period ranges from 7 to 18 days • Prodrome typically includes fever, cough, coryza, conjunctivitis and Koplik spots on the buccal mucosa • Red blotchy rash appears around the 3rd day of illness, beginning on the face and becoming generalized • Maybe complicated by middle ear infection or diarrhea • Severe complications include pneumonia & encephalitis leading to death in approximately 2 /1,000 cases • Most common among children, but also seen in nonimmune adults
CDC- Case Definition • The diagnosis of measles should be considered in any person with a: • generalized maculopapular rash lasting ≥ 3 days • a temperature ≥ 101ºF (38.3ºC) • and cough, coryza, or conjunctivitis • Immunocompromised patients may not exhibit rash or may exhibit an atypical rash • Newborns receiving maternal antibody and people who have received IsG can have an atypical presentation (rash progresses in opposite fashion)
DOH Measles Case Classification • Suspected: Any febrile illness accompanied by a rash • Probable: A case that meets the clinical case definition, has noncontributory or no serologic or virologic testing, and is not epi linked to a confirmed case • Confirmed: A case that is lab confirmed or that meets the clinical case definition and is epi linked to a confirmed case
Preventing Transmission in HC Settings • Suspected patients should be removed from waiting areas as soon as they are identified and: • Placed in a private room with the door closed • Asked to wear a surgical mask • In hospital settings, suspect patients should be placed immediately in a negative-pressure isolation room • Do not send patient to other parts of the hospital for examination or testing • All HC personnel should have documented evidence of measles immunity on file at their work location • Draw blood samples for serologic evidence of immunity when documentation is not available • Vaccinate personnel without evidence of immunity • http://www.cdc.gov/ncidod/dhqp/gl_isolation.html
CDC Recommendations • Case investigation and vaccination of household or other close contacts without evidence of immunity should not be delayed pending the return of lab results • Isolate known and suspected case-patients • Administer vaccine • Immune globulin within 6 days of exposure, particularly contacts ≤ 6 months of age, pregnant women, and immunocompromised people • For contacts who were not immune at the time of exposure: • Exclude from day care, school, or work • Home quarantine from 7 to 21 days following exposure • Persons who are known contacts of measles patients and who develop fever and/or rash should be considered suspected measles case-patients and be appropriately evaluated by a HC provider • If HC providers are aware of the need to assess a suspected case, they should schedule the patient at the end of the day after other patients have left the office and inform clinics or emergency rooms if they are referring a suspected measles patient for evaluation so that airborne infection control precautions can be implemented prior to their arrival
CDC- MMR During Outbreaks • During a measles outbreak, additional vaccine recommendations should be considered: • Children ≥12 months should receive their 1st dose of MMR vaccine as soon after their 1st birthday as possible & their 2nd dose 4 weeks later • Coordinate with neighboring counties • Provide 1 dose of MMR vaccine to unvaccinated HC personnel born <1957 who don’t have serologic evidence of immunity or medical documentation of measles disease • 1 dose of MMR vaccine should be considered for infants ≥ 6 months of age
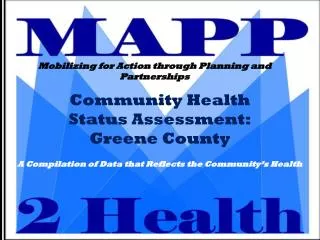
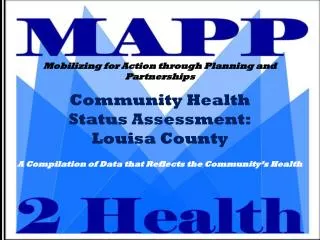
Whatcom San Juan Pend Oreille Ferry Skagit Okanogan Island Clallam Snohomish Stevens Jefferson Chelan Kitsap Douglas King Lincoln Spokane Grays Harbor Mason Grant Kittitas Pierce Thurston Adams Whitman Pacific Lewis Franklin Garfield Yakima Wahkiakum Cowlitz Columbia Walla Walla Skamania Asotin Benton Clark Klickitat <2.0% 2.0-2.9% 3.0-3.9% 4.0-4.9% 5.0% WA State Counties’ School Exemption Rates 2004 Source: WA State Department of Health
Grant County Measles OutbreakCase Investigation • First 2 cases attended Generation Conf in Kirkland, WA-March 27-29, 2008 • Conference hosts Jr High – University students • 3,000 students • 12 states, Japan, Mexico, Canada • No other country, state or county reported measles in attendees • CDC reports measles endemic in Japan
Grant County Measles OutbreakCase Investigation • Index case was home schooled • During infectious period case-patient also: • Attended Church Youth Group • Taught Bible Study • Attended piano lessons • All 7 siblings developed measles • 3/7 developed pneumonia • Neither parent became ill • 2nd case that attended the Generation Conference: • Developed rash one day after 1st case • Attended a Christian School in Moses Lake • Attended same church Youth Group as index case • Subsequent 15 cases could be linked to these 2 families through school or religious activities
Grant County Measles OutbreakAerosol Transmission • One case attended piano lessons with 2 siblings during infectious period • All 3 left residence after piano lesson • Unvaccinated 12 yo child entered home within 1 hour • 12 yo also attended the same school as Case#2 • 12 yo developed measles within 2 weeks • 2nd unvaccinated child entered the same home >2 hrs after 3 siblings departed • Child never developed measles • Unvacc nephew of 12 yo developed measles
Grant County Measles Outbreak18th case • Traveled to Oregon with one parent, one unvacc sibling and one partially vacc sibling • Diagnosis made in Oregon ED due to history of family’s recent travel from Moses Lake • Oregon HO and nurse traveled to family’s temporary residence • Parent ordered to remain in OR • Grant Co HO Directive placed at ML residence • ML contact tracing yielded 2 babysitters, family, and Bible Study attendance • Same Bible Study that the 1st case attended, although not at the same time
Grant County Measles Outbreak19th case • 23 yr old • Educated in Grant County • 2 X MMR • Enrolled in military post HS graduation • Dx: ITP • Splenectomy • Military discharge 2003 • IgG negative • 2 siblings worked at Wal-Mart in ML • Case-patient visited store during infectious period
Grant County Measles OutbreakCommercial Cooperation-19th case • Case-patient entered Wal-Mart during infectious period • A good working relationship was developed with local Wal-Mart managers • Corporate Wal-Mart did not know or use appropriate communication channels. They also contacted legislator(s) about the local HO applying stricter guidelines than they found on the internet (requirement of second MMR to return to work) • Public media release • List of all employees working during that period and 2 hours subsequent • Approx 200 employees who could not prove immunity were vaccinated or titered • Commercial lab increased throughput and released results directly to GCHD • This resulted in expedited return rate to work • Store did not have to be closed
Grant County Measles OutbreakMoses Lake, Washington • 19 case-patients resided in Moses Lake • 12/19 infected by siblings • Age range = 9 months to 23 years • Female = 52.6% ; Male = 47.4% • Highest temp = 103.4F • 18/19 cases unvaccinated • Genotype = D5 • Switzerland, Germany, Japan, AZ • 26 other patients ruled out
Grant County Measles OutbreakHO Directives & Quarantine Orders • Directive required to obtain Generation Conference participant list of approx 60 students/chaperones • HO Directive required to obtain list of Bible Study participants • Quarantine order required for 21 days if: • Direct exposure + no MMR or immunity documentation • Direct exposure + receive 1st MMR plus work in high risk category • High risk defined as HC worker, school teacher, EMT, retail, etc • Rash Watch=255 persons (English, Spanish, & Russian) • Form developed • Required daily call by GCHD staff
Grant County Measles Outbreak17.3% increase in full immunity from May 13th to June 20thTotal Number of Persons = 1075IgG positive = 223
Grant County Measles OutbreakPrimary Case ContactsTotal Number of Persons = 1075
Grant County Measles Outbreak School TypeTotal Number of Persons = 325
Grant County Measles OutbreakContact Investigation ActivitiesTotal Number of Persons = 250
Grant County Measles OutbreakChild Profile • Adult vs peds immunization history • Most adult imms records were difficult to locate • Most imms records for young WA State children were available • Missing imms records were obtained from HC providers or schools • Titers were provided at low cost by Samaritan Healthcare • All titer and imms results were entered into CP by GCHD staff • Rapid access to records resulted in a fast return to work or school
Grant County Measles Outbreak Healthcare Facilities • Response: posted signs on all doors indicating those with rash and fever can not enter without mask • If the patient contacted PH first we screened the cases • Those who required immediate HC were told to call provider first • Facilities provided lists of employees and patients who were present 0.5 hr before and 2 hrs after case-patient • Hundreds of people were screened for each case-patient
Grant County Measles OutbreakHC and Media Releases • Periodic Emails/fax to HC providers, EMS • Media releases to keep public informed • All media releases posted at www.granthealth.org • July 22nd- “Grant County measles outbreak may be over”
Grant Co. Measles OutbreakLessons Learned • Provide timely written notification of any HO requested or ordered restriction; delivering them in person is effective • Hold daily update meetings with staff – both offices • Work closely with commercial labs to assure “collection” of all suspect patients and to obtain rapid results • Moses Lake bus station was not able to support transport of specimens, had to take them to Ellensburg (extra driving) • Negotiate a specific time to provide updates to DOH • ICS-like structure was utilized; increased specificity of assignments with actual ICS would have been helpful • Using one office for measles EOC and the other one for other routine PH including most immunizations was helpful, especially during concurrent Varicella outbreak measures • One clinic made an isolated location available for collecting lab samples, for their own and other patients • Specific extension was set up for a "measles hotline”; prioritizing those and other voicemails was helpful
Expense • HO • Attorney • GCHD staff • Regional Epi • Vaccine, IsG