What We Know
This initiative aims to address significantly higher rates of adverse birth outcomes and maternal mortality among African American women. Traditional prenatal care has proven insufficient, necessitating a revised model that integrates social factors and community support. The program emphasizes empowerment, self-efficacy, and comprehensive group interventions to enhance health behaviors and social connections. By addressing systemic inequities and fostering collaboration among providers and communities, the goal is to reduce disparities and improve health outcomes for African American mothers and infants in California.

What We Know
E N D
Presentation Transcript
What We Know Paula Braveman, MD, MPH Reggie Caldwell, LCSW
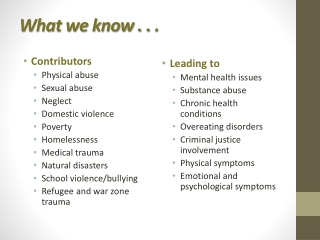
The Problem • 2-3 times higher rates of adverse birth outcomes among African American babies • 4 times higher ratio of maternal mortality among African American women • Traditional prenatal care has not improved birth outcomes • but some promising results from Centering Pregnancy
The Science • The birth outcome patterns suggest that social factors are involved. Prime suspects include: • Stress – especially chronic, e.g., due to discrimination &/or economic hardships ; plausible physiologic pathways • Social support may directly improve health; affects health behaviors; buffers stress effects • Empowerment --Self-efficacy plays key role in health behaviors; key to escaping poverty; lack of control at work strongly linked with heart disease • Empowerment-focused group approaches may be more effective than 1:1 (based on theory and data) • In other words: SSE WAS ON THE RIGHT TRACK!
Rationale for Revising BIH • Great work happening, but varied across sites so impossible to evaluate impact • Bring BIH up to date with science • More emphasis on systematically addressing social factors as key determinants of health and health behaviors • Focus efforts to maximize impact
The Revised BIH Model • Combined the best of original BIH models with promising practices: Amplified SSE strength-based group intervention, supported by empowerment- & referral-oriented case mgmt • Goal: Decrease disparities by improving African American infant and maternal health • May not be able to see a difference in birth outcomes, especially short-term • But current science tells us that at the least, if we focus, we can strengthen maternal capacity, behaviors, & social support, which should improve maternal and infant health
Conceptual Framework Intermediate Outcomes BIH Activities • INDIVIDUAL • Increased health knowledge • Increased healthy behaviors • Increased empowerment through improved life skills and coping skills • Increased receipt of quality medical, social & mental health services • Decreased unplanned pregnancy • Increased social support both for & among the women • Decreased stress by mobilizing resources and services • Improved parenting • Increased bonding between mother & infant • Improved infants’ developmental milestones • COMMUNITY • Increased community and provider knowledge & cultural competence • Increased community partnerships & linkages among service agencies • Decreased stressors in the community through community & provider/agency action • Improved understanding among community and providers of influence of social inequities on health • INDIVIDUAL • Services provided to African-American women, infants, and their families & partners include: • Referrals to medical, social & mental health services • Health education • Social and group support • Identifying resources • Self-advocacy • COMMUNITY • Promote community and provider engagement and advocacy • Educate community and providers about influence of social inequities on health Problem • Poor birth outcomes • Social isolation • Lack of health knowledge • Lack of access to quality health care • Poverty • Racism • Environmental stressors • Maximizing impact of the program (numbers served & effect size) • Lack of cultural awareness and skills among providers Ultimate Goal To improve African American infant and maternal health in California and decrease Black:White health disparities and social inequities for women and infants GUIDING PRINCIPLES 1. Comprehensive and integrated: Address multiple risk factors and use multiple strategies 2. Multi-level: Address individual, community, service systems and societal levels, with empowerment focus 3. Collaborative: Partner with community providers and agencies with similar activities 4. Community-driven: Developed, implemented and evaluated by local communities 5. Evidence-based: Developed from proven or promising strategies; impact is measurable 6. Culturally competent: Designed & implemented in a culturally-competent manner 7. Staff training and professional development: Conducted to ensure the BIH activities are provided effectively DRAFT
To Impact Maternal & Infant Health, BIH Needed To: • Decrease isolation/increase social support • Build self-esteem and empower women to make better choices about their health • Decrease stress/improve coping skills • Involve communities
Program Tenets • Promote and support healthy pregnancy and parenting. • Build on client’s strengths to enrich them, their families and their community by empowering them to make healthy decisions • Culturally relevant and honor the unique history and traditions of people of African descent • Address issues important to African American women • Reduce disparities by improving African American maternal and infant health.
Black Infant Health Program - Revised Model Recruitment Meets program requirements? Standardized health promotion message & Refer out to appropriate agency No Yes • Intake • Program orientation and consent • Referrals • Prenatal Assessment 1 • Initiation of Individual Client Plan (ICP) • Case Conferencing Core Intervention Group Sessions 1-10 Prenatal Case Management that compliments the group sessions Birth Group Sessions 11-20 Postpartum • Program Completion • Complete ICP • Complete Life Plan • Complete Case Closure
Groups • Use facilitative learning to access and enhance women’s knowledge and skills • Group format means women draw strength from each other • Skill-building to achieve better physical and mental health • Weekly personal goal setting culminating in the creation of a Life Plan • Focus on empowerment to: • Make good choices to have a healthy pregnancy • Be a good role model for one’s child.
Challenges Identified • Staff • Resistant to change • Reluctant about the revised model’s success • Great facilitation • Focused on “What If’s” • Clients • Retaining them in groups (transportation and child care issues) • Motivation for long-term participation/competing priorities
Themes from theProgress Report Successes Challenges Some staff are having difficulty embracing the new model New data book Client transportation Time for case conferences and other staff meetings Serving clients with multiple stressors • Collaborations with providers, community partners, and Board • Received or applied for a grant • Positive feedback from clients about new model • In-kind donations • Flexibility by training all staff as group facilitators
The “Magic” is Happening Staff Clients A place where negative messages are countered with positive ones I now have a vision for my life The group constantly reminds me that we ALL have talent • I learn about myself while I conduct the group • It’s challenging and worth it! • I used harm reduction strategies to help a pregnant client stop smoking How to we keep the “magic” going?