Download
1 / 29
290 likes | 690 Views
Massive Transfusion and Dubbo. Anand Rajan Anaesthetic Registrar, POWH and DBH. Overview. Initial Concepts Haemorrhage Shock Traumatic Shock Diagnosis/monitoring bleeding Available blood products and treatments DBH Massive Transfusion Protocol Incident reporting. Definitions.

E N D
Massive Transfusion and Dubbo Anand Rajan Anaesthetic Registrar, POWH and DBH
Overview • Initial Concepts • Haemorrhage • Shock • Traumatic Shock • Diagnosis/monitoring bleeding • Available blood products and treatments • DBH Massive Transfusion Protocol • Incident reporting
Definitions • Haemorrhagic: derived from Greek "haima," blood + rhegnumai," to break forth = a free and forceful escape of blood • Classification from American College of surgeons • Shock: a condition of decreased total body oxygen delivery • Massive Transfusion: • several definitions • from ARCBS: • replacement of the patient’s entire blood volume within 24 hours,or • more than 20 units of red cells transfused within 24 hours. • Other definitions: • 50% blood volume loss in 3 hrs • Rate of blood loss>150ml/min • Need for >8-10u RBC
Shock • Types include: • Hypovolaemic:loss of circulating fluid volume • Cardiogenic:failure of the heart to pump blood through the body • Neurogenic:loss of vascular tone • Anaemic:decreased oxygen carrying capacity • ‘Traumatic shock’ • Combination of these • Haemorrhagic, anaemic ± cardiogenic/neurogenic phases • Clinically different presentation from laboratory-produced haemorrhage
Traumatic Shock • Phases: • Compensated • Tachycardia • Circulating blood diverted to critical circulations • Decompensated • Ischaemia creates an O2 debt • Shock is still reversible • Subacute irreversible • Can be haemodynamically resuscitated • Risk of multi-organ failure from prolonged ischaemia • Acute irreversible • Spiral of • Haemorrhage • Acidosis • Coagulopathy • Cardiovascular collapse and death
Bodily response to shock • At a macrovascular level: a neuroendocrine response: • Fluid shifts: • Vaso/veno-constriction • Diversion of blood to cardiac/cerebral circulations • Fluids drawn from interstitial to intravascular space • Sympathetic response(In concert with above) : • Aim to maintain mean arterial pressure • Renal effects retain fluid and produce oliguria • Assist fluid shift • Cellular level: • Coagulation initiated • Ischaemic effect: build-up of lactate (anaerobic metabolism), cytokines and other pro-inflammatory mediators
Haemostasis • Physiological mechanisms to minimise blood loss from damaged blood vessels • Primary haemostasis: platelet-mediated (soft plug) • Secondary haemostasis: coagulation cascade (definitive clot) • (But, these occur simultaneously)
Coagulation Cascade • Pathways: • Intrinsic • Initiated by non-endothelial surfaces interacting with factor 12 • Extrinsic • More important in haemostasis • Release of thromboplastin in response to tissue trauma • Activates factor VII, initiating the sequence • Final common pathway with activation of Factor 10 • Simultaneous fibrinolysis to limit response and retain vascular patency
Aggressive fluids and transfusion • Confronted by: • Hypovolaemia • Hypothermia • Coagulopathy • Hypocalcaemia • Hyperkalaemia
Why does acute traumatic coagulopathy occur? • Traditional belief: • Consumption of coagulation factors • Dilution from IVF therapy • Hypothermia • Metabolic acidosis • New concepts • Hypoperfusion triggers the anticoagulation thrombomodulin protein C pathway • This plays the central role • Protein C • limits thrombin production (preventing further clot formation) • resolves already formed clots (hyperfibrinolysis) • Adverse associations: Increased mortality, blood transfusion requirements, ARF, reduced ventilator-free days post trauma
Diagnosis/monitoring bleeding • Assessment of haemorrhage and volume status • Clinical parameters • HR/BP • Non-specific • Central/mixed venous saturations • Require central access • More reliable measure of acute volume loss • Arterial blood gas sampling • Helps evaluate degree of shock • Base deficit: shown to correlate with • Transfusion requirements • ICU stay • Ultimate Outcome • Lactate: ability to clear to normal = ‘one of the most important predictors of survival following haemorrhage and injury’
Diagnosis/monitoring bleeding • Assessment of coagulation: • Prothrombin time • Measure of extrinsic pathway • Measures Factors II, V, VII, X, fibrinogen • Standardised by International Normalised Ratio (INR) • Activated partial thromboplastin time (APTT) • Measure of intrinsic and common coagulation pathways • Measures factors VIII, IX, XI, XII • Other tests: Platelet count, Hb, fibrinogen levels
Diagnosis/monitoring bleeding • Questionable value of tests: • Delays to obtaining results (45-60 mins) • Coagulation tests performed in plasma (vs whole blood) • No information available re platelet function • Assays are performed at T=37º rather than patient temperature • Still important to take tests but clinical picture will have changed by the time results arrive
Treatment • Minimise initial phase after trauma • Prevent bleeding • Prompt surgical referral • Target systolic BP 80-100mmHg until major bleeding is stopped • Above BP target applicable if no brain injury • Currently aim for aggressive fluid therapy • ?Low-volume resuscitation • Not in brain and spinal injuries • IVF and blood products
Have you given blood products yet? Which one do I give? Are you telling me you’ve waited this long?
Other complications & the ‘storage lesion’ • Preservatives needed to maintain 70% cell viability at 24 hours (storage up to 42 days) • Addition of: Citrate (anticoagulant), Phosphate (buffer), Dextrose (glucose source) and Adenine (ATP substrate) • Effects of the storage lesion: • There is a need for specific goal-directed transfusions, with the help of clinical algorithms
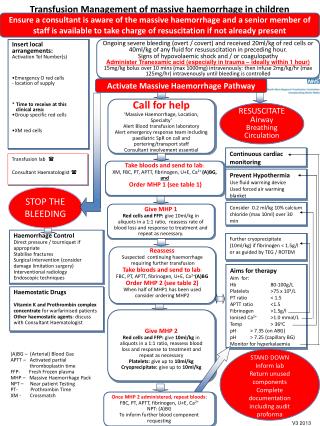
CRITERIA Ongoing bleeding with any of: 1. Trauma patients with life-threatening haemorrhage. 2. Expected replacement of >1 blood volume in 24 hrs / 50% blood volume loss within 3 hours / rate of blood loss of >150ml/min. 3. Ongoing bleeding after 4 units of packed cells have been transfused within 4 hours. ACTIVATION - The most senior clinician involved in resuscitation contacts pathology/lab scientists to activate the protocol when above criteria are met. - If the protocol is activated the laboratory scientist should record the name of the medical officer, and dispense blood component as per the massive transfusion protocol pack (see below). - Laboratory scientist to remain on site until medical officer allows him/her to go. MASSIVE TRANSFUSION PROTOCOL PACK - 4 units Packed Red Blood Cells (PRBCs), 4 units FFP, 10 cryoprecipitate (MTP 1) Alternating with: - 4 units PRBCs, 4 units FFP, 4 units platelets (MTP 2) - Suggest additional - platelets: if platelets <50 x 10/L or <100 x 10/L with head injury - cryoprecipitate: if fibrinogen <1g/L - FFP: if PT, APTT prolonged and provided that fibrinogen is >1g/l - PRBCs – if Hb <80g/L (may vary in different clinical scenarios) MANAGEMENT OF MASSIVE TRANSFUSION • Haemorrhage control: early consultant input to control bleeding • Prevent Hypothermia (or correct): Active patient warming and fluid warming are essential. Monitor core temperature - either rectal or nasopharyngeal. • Prevent Hypocalcaemia (or correct): check Ca++ regularly and replace as required. • Haematological Tests Hourly: FBC, Coags, Fibrinogen. Send specimens at regular intervals but do not delay transfusion of blood products while waiting for results. Inform laboratory that urgent coagulation testing is required with results rung through to the point of care. • Blood gas analysis: at least hourly to monitor acid-base status and Ca++. • Blood bank will not thaw frozen products in advance so provide resource and time for products that need to be thawed. FACTOR VIIa • Give 90 mcg/kg if ongoing bleeding (at managing consultants discretion). • Round dose up to nearest ampoule to avoid wastage. e.g. 60 kg dose is 5.4 mg but give 6.0 mg (4.8 mg amp plus 1.2 mg amp) • Repeat dose every 2 hours while bleeding not controlled. • Note that FVIIa is unlikely to be effective without adequate replacement of platelets and fibrinogen. Please note that pathology services are on site from 8:30am to 7:30pm on weekdays, and 8:30am to 5:30pm on weekends. Please ensure that blood is sent as early as possible for cross-matching. In order to call pathology services in to the hospital after hours, or to obtain FVIIa call the After Hours Nurse Manager (phone – 0429 601 811, page 104). This Massive Transfusion protocol has been developed to ensure timely and adequate availability of blood and blood products and appropriate replacement of clotting factors. Please fill in an incident report regarding any massive transfusions that have taken place so that procedure can be reviewed. DBH MBT Protocol
After the event • Incident Reporting: • Review: • Incident • Processes following the incident • Massive transfusion • Root Cause Analyses: • Aim to • Ascertain/analyse the cause of problems (ie not symptomatic treatment) • Determine solutions or preventative measures • Many different methods exist • Disadvantages: often related to RCA method used • Choice of investigator: suitability, potential for bias to re-direct investigation • Training of investigators familiar with processes • Possibility that a clear cause is not identified
Summary • Ongoing haemorrhage increases risk of irreversible traumatic shock and may produce a need for massive transfusion • Management requires an interdisciplinary approach • Complications exist from administering large volumes of individual blood products • Therefore massive transfusion protocols involve regimens using multiple blood products, with regular blood testing • Importance of lab staff awareness of massive transfusion requirements in order to expedite products, and importance of medical/nursing staff to inform lab staff of this need • Ongoing review of the process after the incident has occurred
References • Australian Red Cross Blood Service: Transfusion Medicine Manual. http://manual.transfusion.com.au/Transfusion-Clinical-Practice/Disease-Therapeutics/Massive-Transfusion.aspx (visited July 2009) • Massive Transfusion and Control of Hemorrhage in the Trauma Patient. The International Trauma Anesthesia and Critical Care Society (ITACCS), 2003. • www.medterms.com (viewed July 2009) • Theusinger O, Saphn D, Ganter M. Transfusion in trauma: why and how should we change our current practice? Curr Opin Anaesthesiol, 22:305-312. • www.rxlist.com (viewed July 2009) • Brunton L, Parker P. Goodman and gilman’s manual of pharmacology and therapeutics. The McGraw-Hill Companies, New York, 2008. • Peck TE, Hill SA, Williams M. Pharmacollgy for anaesthesia and intensive care, 3rd edition. Cambridge University Press, Cambridge, 2008. • Kleinman S. Massive blood transfusion. UptoDate, Oct 2008.