Download
1 / 39
490 likes | 1.29k Views
CADASIL. Mary Quiceno, M.D. Clinical Assistant Professor Department of Neurology UT Southwestern Medical Center. Neuropathology report on NP36015. What is CADASIL?. C erebral A utosomal D ominant A rteriopathy with S ubcortical I nfarcts & L euko-encephalopathy.

E N D
CADASIL Mary Quiceno, M.D. Clinical Assistant Professor Department of Neurology UT Southwestern Medical Center
Neuropathology report on NP36015 What is CADASIL?
Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts & Leuko-encephalopathy Inherited small vessel disease causing stroke and subcortical vascular dementia that starts in early adulthood and progresses over time. This is a nonatherosclerotic, nonamyloid angiopathy involving small arteries and capillaries of the brain and other organs. Caused by missense mutations in the Notch3 gene on chromosome 19p13. CADASIL
CADASIL • 1977: family w/hereditary, multi-infarct dementia syndrome • Presents in mid-20s to age 45 • Stroke, dementia, migraine with aura, mood disorders • Shortened life span • Most die by age 65 • Unknown prevalence • 400 families world-wide • 2/100,000 • Largely undiagnosed
Case Studies • Most reported cases from Europe • 105 people from 33 affected families • Vascular risk factors are uncommon • Mean age of initial symptom onset 36 + 12 years • Migraine in 40% (28 + 11 yrs) • Stroke/ TIA 43% (41 + 9 yrs) • Depression 8% • Cognitive decline 6% • Seizure 3%
overall, 67% had a TIA or stroke • overall, 42% had dementia • >30% with migraine w/aura and 15% w/mood d/o • overall, age of death, in the 20% of the cohort that was deceased, was 54.8 + 10 years • Course is heterogeneous even in the same family: some remain asymptomatic until their 70s whereas others are severely affected by the age of 50.
MIGRAINE with aura • Often initial feature • 1/3 of families • Occurs earlier as compared to stroke • Consider CADASIL in migraineur with diffuse white matter lesions on MRI • Not small, scattered hyperintensities, which can be seen in migraineurs (16%) who don’t have CADASIL
STROKE • TIAs and subcortical ischemic strokes • Accumulating sensory, motor, and cognitive deficits • Most common feature • Typical stroke risk factors NOT present • Cerebral non-atherosclerotic, nonamyloid angiopathy • Primarily affecting small vessels that penetrate white matter and basal ganglia
MOOD DISORDERS • Depression • Bipolar disorder • Like migraine, CADASIL should only be considered when MRI changes are present • Tend to predate cognitive decline
29 yr old son 4th psychiatric hosp. admission Depression and psychosis 52 yr old father Migraines, stroke Antisocial and withdrawn 72 yr old paternal grandmother Depression at age 50 Dementia at age 61 Frontal lobe dysfunction Retrieval deficits Mood Disorders in an affected family
COGNITIVE DEFICITS • Slowly progressive in addition to stepwise deterioration • Typically appears after stroke symptoms appear • Can be presenting feature • Frontal lobe dysfunction • Memory impairment • Pseudobulbar palsy, gait disturbances, pyramidal signs, sphincter incontinence • Subcortical dementia • Vascular dementia
Cognitive profile • CADASIL compared to normals • Impaired on executive function and speed measures • Delis-Kaplan Executive Function System (D-KEFS) • Trails motor speed subtest from the D-KEFS • CADASIL w/stroke and cerebral small vessel disease (SVD) • SVD typically older • Both impaired similarly on executive fx and speed • CADASIL worse on verbal fluency (letter)
Executive Function • refers to a wide range of central control processes in the brain that connect, prioritize, and integrate operation of subordinate brain functions • this central management system, often attributed to operations in the prefrontal cortex, is crucial to organizing and integrating cognitive processes over time and plays an increasingly important role as we mature • organizes, activates, focuses, integrates, and directs • Executive functions require several higher-level cognitive abilities for successful performance. • These can be assessed with tasks that require: • – initiation of effortful and novel thinking • – isolation of a common feature or attribute from among the array of target stimuli • – formation of a higher-level concept that captures the defining properties of those common features • – flexibility of thinking in order to abandon one conceptual relationship in order to apprehend new ones
Other organ disease • In some patients w/CADASIL • silent retinal microvascular circulatory changes • 18 pts: No visual symptoms. VA was normal in all. Ophthalmologic abnormalities were found in 8 patients. • FE and FA revealed silent retinal abnormalities in CADASIL patients with nerve fiber loss in 22% and cotton wool spots in 17%. • may be considered as peripheral markers of this genetic disease. • high frequency of myocardial infarction in a single series of Dutch patients • Distinct from CADASIL, hereditary endotheliopathy with retinopathy, nephropathy, and stroke (HERNS) is an autosomal dominant multi-infarct syndrome with systemic involvement.
Brain Imaging in CADASIL • Diffuse white matter hyperintensities on T2 and FLAIR weighted images • Subcortical white matter • Basal ganglia • Changes on MRI may be evident in persons who are in their 20s • Penetrance complete by age 35 and all will have MRI findings • The syndrome may not be suspected until affected individuals are in their 50s or older • Lesion volume is inversely correlated with cognitive function
MRI Changes • Axial FLAIR images • 59 yr old woman • Multiple confluent hyperintensities in deep and periventricular white matter
MRI • Most specific finding to differentiate CADASIL from ischemic leukoaraiosis • T2 hyperintenisties in anterior temporal pole
MRI in CADASIL w/characteristic MRI findings of involvement of the external capsule and anterior temporal lobes.
Differentiating CADASIL from other diseases affecting the white matter • Ischemic small-vessel disease • Usually occurs after fifth decade • Vascular risk factors present • Multiple Sclerosis • More likely to see spinal cord and corpus callosum lesions • Periventricular lesions are ovoid and/or oriented perpendicular to lateral ventricles
When to consider MRI in migraineur • Consider MRI if • Migraine attacks with aura begin in mid-adulthood • Atypical aura • Hemiplegic, basilar, prolonged • Family history of stroke, dementia, depression • Focal neurological signs
When to Suspect CADASIL • Recurrent subcortical ischemic strokes • Esp. <60 yrs old • Esp. in absence of vascular risk factors • Early cognitive decline • Migraine with aura • Comorbid psychiatric symptoms • Depression • Bipolar
When to Suspect CADASIL • Abnormal MRI • Significant white matter lesions before age 35 • Multiple T2 hyperintensities w/o vascular risk factors • Bilateral T2 hyperintensities in white matter, esp. w/lesions in ant. Temporal poles • Family history • Stroke, dementia, depression, migraine w/aura, other white matter diseases (which may be misdiagnosed) • Premature CAD
Diagnostic Approach • History • MRI with involvement of anterior temporal poles OR external capsule *** & • Positive gene testing *** • Sensitivity of 100% with Hx, MRI, & gene test in one study from England
Biopsy • Skin biopsy was positive in approximately half of the 18 patients tested • Skin biopsy was negative in all of the gene negative patients • Sensitivity of 100% • Granular osmiophilic material seen on EM • Sensitivity 50%, specificity 100% • Tissue samples stained with monoclonal Ab top Notch3 protein • Sensitivity 96%, specificity 100%
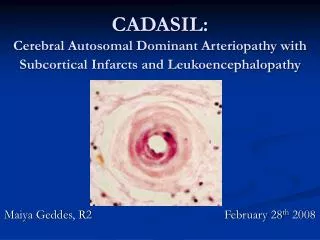
The hallmark of the disease is the presence of granular osmiophilic material which is seen adjacent to the basement membrane of the smooth muscle cells of arterioles on electron microscopy. • This is pathognomic for CADASIL. • The deposition of GOM in skin arterioles may vary depending on the exact mutation involved. • The vascular defects are present in every tissue and may be detected histologically by examining arterioles in skin biopsy, where accumulation of granular and osmiophilic material within the smooth muscle cell basement membrane and the surrounding extracellular matrix.
Blood vessels in CADASIL • w/ basophilic granular material (below) • EM (to right)
2 types of changes in arteries, veins in body Basophilic degeneration and thickening of the media (top picture) Fibrinoid necrosis of the media sometimes associated with delicate perivascular inflammatory infiltrates (bottom picture) Blood vessels in CADASIL
Notch3 ab in brain blood vessels • Notch3 immunoreactivity in vascular smooth muscle cells • Normal controls on left (a, c, e) • CADASIL patients on right (b, d, f)
What leads to CADASIL? • Mutations in notch3 gene • Odd number of cysteine residues in Notch3 receptor extracellular domain • Impaired clearance of cleavage product • Alterations of vascular smooth muscle • Presence of granular osmiophilic deposits
Notch3 gene mutation • Usually missense mutation • More than 50 have been found • Spontaneous mutations have been described • The protein folds incorrectly • Leads to accumulation of protein in membranes of smooth muscles and, ultimately, fibrosis and luminal narrowing of them
Notch3 gene • Mutation in Notch3 gene on chromosome 19 • Just downstream from a mutation found in familial hemiplegic migraine • Notch 3 gene encodes a transmembrane receptor • Functions in signaling pathways essential for maturation of blood vessels • In adults, it is maximally expressed in vascular smooth muscle in small to medium arteries • Interaction of notch receptor with its ligand leads to cleavage of the transmembrane receptor which migrates into the nucleus and, associated with a transcription factor, activates transcription of primary target genes.
The notch in the Drosophila wing • In fruit fly heterozygotes for Notch3 gene have a “notch” in their wing • The mutation is lethal in homozygotes • Notch proteins • Encode transmembrane receptors involved in determination of cell fate during development • Proliferation, differentiation, apoptosis
Pathogenic Hypothesis • Notch 3 expression is limited to vascular smooth muscle cells • Mature vascular smooth muscle cells require continued function of the Notch 3 pathway • Continued survival • Blood vessels are narrowed and weak and do not react to fluctuations of CO2 and BP • Capillaries, veins are involved • Generalized vasculopathy
Brain Predilection • Cerebral vessels have fewer smooth muscle cells than vessels of other organs • Increased susceptibility • Limited ability for regeneration of CNS tissue • White matter predilection • Insufficient collateral circulation • Density less than in grey matter
What can be done for these patients? • Treatment • Control vascular disease risk factors • BP • Increased SBP independent risk factor for progression of CADASIL • Cholesterol • DM • Smoking • Obesity • Avoid OCP, HRT
Treatment • Antiplatelet therapy • Investigate for other causes of stroke (cardiac, afib, hypercoag state, etc.) • Cholinesterase inhibitors • Work in vascular dementia • Screen for mood disorders, cognitive decline, seizure • Life expectancy may be shortened by 6 years
NP36015 • The key finding • Abundant basophilic (blue on H&E), PAS positive, osmiophilic (black on EM) granular material seen in the markedly thickened blood vessel walls • Differential diagnosis • Atheroscerotic disease • Blood vessel walls are also thickened • Granular material is not usually present (if present, it differs from that seen in CADASIL)
No treatment • Screening not indicated, unless family member is affected • Family may wish to seek genetic counseling • Control vascular risk factors • Do not smoke • Screen for mood disorders, cognitive decline, focal neurologic signs, seizure