Download
1 / 29
470 likes | 1.79k Views
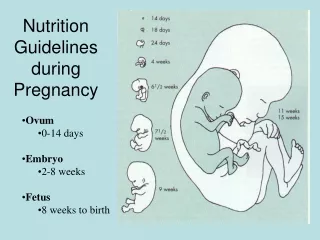
SAGES Guidelines for Laparoscopic Surgery During Pregnancy. Steven J. Heneghan MD FACS Director Mithoefer Center for Rural Surgery Surgeon in Chief Bassett Healthcare. The SAGES Guidelines for the Diagnosis, Treatment, and Use of Laparoscopy for Surgical Problems During Pregnancy.

E N D
SAGES Guidelines for Laparoscopic Surgery During Pregnancy Steven J. Heneghan MD FACS Director Mithoefer Center for Rural Surgery Surgeon in Chief Bassett Healthcare
The SAGES Guidelines for the Diagnosis, Treatment, and Use of Laparoscopy for Surgical Problems During Pregnancy Raymond R. Price MD Vice-Chairman Dept of Surgery Intermountain Medical Center Intermountain Healthcare Adjunct Assistant Clinical Professor of Surgery University of Utah Heidi Jackson MD Steven Granger MD Michael Rollins MD Robert Fanelli MD William Richardson MD David Earle MD
Guidelines • There is a considerable amount of effort toward standardizing guidelines • Rating the evidence • Rating the recommendations • Avoiding using guidelines to reduce professional competition and a move to having them a resource for both patients and clinicians • There is an effort to have agreement between organizations with regard to guidelines.
22 References * 8 guidelines 175 References * 23 guidelines Guidelines for Laparoscopic Surgery During Pregnancy* SAGES 1996 Guidelines for Diagnosis, Treatment, and use of Laparoscopy for Surgical Problems During Pregnancy* 2007
Scale for Evidence Grading High-level (level I or II), well-performed studies with uniform interpretation and conclusions by the expert panel Grade A High-level, well-performed studies with varying interpretation and conclusion by the expert panel Grade B Lower level evidence (level II or less) with inconsistent findings and/or varying interpretations or conclusions by the expert panel Grade C
Guidelines Imaging • 1 Ultrasonographic imaging during pregnancy is safe and useful in identifying the etiology of acute abdominal pain in the pregnant patient Level II Grade A • 2 Expeditious and accurate diagnosis should take precedence over concerns for ionizing radiation. Radiation dosage should be limited to 5 to 10 rads Level III Grade B • 3 CT delivers 2-4 rads which falls below the limit and may be considered an appropriate test Level III Grade B
Guidelines Imaging • 4 MR Imaging can be performed without IV Gadolinium Level III Grade B • 5 Nuclear medicine administration of radio nucleotides can generally be done at safe levels Level III Grade C • 6 Intraoperative Cholangiography exposes the mother and fetus to minimal radiation and may be uses selectively during surgery. Level III Grade B
Changes in Recommendations 1996 2007 Pre- and post-operative Monitoring Fetus Intra-operative Second trimester deferment Trimester 2nd 1st, 2nd, 3rd 8-12 mm Hg 10-15 mm Hg Pneumoperitoneum Serial maternal ABG/ ETCO2 Intra-operative Monitoring ETCO2 30-40 Open (Hasson) or Closed (Verres) Abdominal Access Open (Hasson)
Clinical Scenario • 24 yo female 12 weeks pregnant • RUQ abdominal pain every 3-4 days • Occurs after fatty meals • US: multiple stones, no wall thickening • Normal LFT’s, amylase, lipase “I was told by another surgeon that because I was pregnant, I could not have laparoscopic surgery.”
Questions? • Should I offer her a cholecystectomy? • Timing of surgery? • Open or laparoscopic? • Monitoring of fetus intraoperatively? • If laparoscopic: • What entry technique should be used? • Port placement? • Appropriate level of pneumoperitoneum? • Patient positioning? • Need for OB consultation? • ERCP or intraoperative cholangiogram?
TocolyticsGuideline 23: Tocolytics should not be used prophylactically, but should be considered peri-operatively when signs of preterm labor are present in coordination with obstetric consultation (Level I, Grade A). $94.8 million awarded to mother of 8 year-old boy. Failure to use tocolytics.
Fetal Heart MonitoringGuideline 21: Fetal heart monitoring should occur pre and postoperatively in the setting of urgent abdominal surgery during pregnancy (Level III, Grade B). No intra-operative fetal heart rate abnormalities reported.
Long term effects on the children? Preterm Delivery Rate? Abortion Rate? Laparoscopy and Trimester of PregnancyGuideline 9: Laparoscopy can be safely performed during any trimester of pregnancy (Level II, Grade B).
Gallbladder DiseaseGuideline 15: Laparoscopic cholecystectomy is the treatment of choice in the pregnant patient with gallbladder disease regardless of trimester (Level II, Grade B). Non-operative Management Symptom recurrence 1st - 92% 2nd – 64% 3rd – 44% Hospitalizations Spontaneous Abortions Pre-term Labor
Initial Port PlacementGuideline 11: Initial access can be safely accomplished with an open or Hassan, Verres needle or optical trocar if the location is adjusted according to fundal height, previous incisions and experience of the surgeon (Level III, Grade B).
Fundal Height by Gestational Age in Weeks 36 40 32 26 20 16 12 8 Rollins MD, Price RR. Laparoscopic surgery during pregnancy. In: Inderbir SG ed. Textbook of laparoscopic urology. New York: Informa Healthcare USA, Inc., 2006:983-986.
Trocar Placement for Laparoscopic Appendectomy 2 1 3 2 1 3 2 1 3 1st Trimester 2nd Trimester 3rd Trimester Changes by size of gravid uterus. Rollins MD, Price RR. Laparoscopic surgery during pregnancy. In: Inderbir SG ed. Textbook of laparoscopic urology. New York: Informa Healthcare USA, Inc., 2006:983-986.
Insufflation PressureGuideline 12: CO2 insufflation of 10-15 mmHg can be safely used for laparoscopy in the pregnant patient. Intra-abdominal pressure should be sufficient to allow for adequate visualization (Level III, Grade C). Maternal Pulmonary Visualization Fetal Acidosis
Maternal Pulmonary Residual Volume Growing fetus Pressure on diaphragm Functional Residual Capacity PaO2 Pressures of 15 mmHg – no increased adverse outcomes to the patient or fetus
Fetal Animal Studies CO2 Pneumoperitoneum Acidosis Tachycardia Hypertension Hypercapnia Devon’s Racing Rams (photo Rick Turner) No evidence to support long term detrimental effects resulting from CO2 pneumoperitoneum in humans
Intra-operative CO2 monitoringGuideline 13: Intra-operative CO2 monitoring by capnography should be used during laparoscopy in the pregnant patient (Level III, Grade C). Maternal arterial blood gas (PaCO2) vs. End-tidal CO2 (EtCO2) Capnography adequately reflects maternal acid/base status in humans.
Clinical Scenario • ER physician calls you to see a 27 year old 8 week pregnant patient with 8 hours of R lower quadrant pain. She has been nauseated for 8 wks. • Abdomen only mildly tender RLQ to deep palpation • WBC 16 US abdomen CT scan Exploratory laparoscopy Possible options:
UltrasoundGuideline 1: Ultrasonographic imaging during pregnancy is safe and useful in identifying the etiology of acute abdominal pain in the pregnant patient (Level II, Grade A). 1. Radiographic test of choice for most gynecologic causes of abdominal pain 2. Useful 1st line diagnostic study for many non-gyn causes
* Radiation dosage < 5 rads minimal fetal risk * Fetal age at exposure 1st week of conception - mortality 10-17 weeks gestation – CNS teratogenesis Later pregnancy – hematologic cancer Risk of Ionizing RadiationGuideline 2: Expeditious and accurate diagnosis should take precedence over concerns for ionizing radiation. Radiation dosage should be limited to 5-10 rads in the first 25 weeks of pregnancy (Level III, Grade B).
Fetal Radiation Exposure from Diagnostic Imaging Studies Study Rads Chest radiograph <0.001 Abdominal series 0.245 Pelvic radiograph 0.04 Upper gastrointestinal series 0.05-0.1 Barium enema 0.3-4 HIDA scan 0.15 Chest CT scan 0.01-0.2 Abdominal CT scan 0.8-3 Pelvic CT scan 2.2 Rollins MD, Price RR. Laparoscopic surgery during pregnancy. In: Inderbir SG ed. Textbook of laparoscopic urology. New York: Informa Healthcare USA, Inc., 2006:983-986.
CT abdomen and pelvis 2-4 rads Computed TomographyGuideline 3: Contemporary multi-detector CT protocols deliver a radiation dose to the fetus below detrimental levels and may be considered as an appropriate test during pregnancy depending on the clinical situation (Level III, Grade B). Early identification Rate of perforation Practitioners should be aware of the radiation doses delivered by the CT scanners in their facilities.
Laparoscopic AppendectomyGuideline 17: Laparoscopic appendectomy may be performed safely in any patients with suspicion of appendicitis (Level II, Grade B).
Conclusions • Guidelines are a moving process and when published they are a point in time rather than a completed process • Guidelines are much more difficult than most people realize • Guidelines should give the references for the conclusions the rating of the references and grading of the recommendations • www.sages.com