Download
1 / 21
210 likes | 330 Views
Critically Appraising the Sexual Health Strategy. Dr Paul Flowers Reader in Psychology Glasgow Caledonian University. Structure of presentation. The strategy as a viable document Confusion surrounding the prioritisation of social versus individual issues

E N D
Critically Appraising the Sexual Health Strategy Dr Paul Flowers Reader in Psychology Glasgow Caledonian University
Structure of presentation • The strategy as a viable document • Confusion surrounding the prioritisation of social versus individual issues • Blurring and tension between socio-cultural and medical/public health perspectives • The loss of focus upon clear target groups • Absences within the strategy
The strategy as a viable document: too inclusive? • It is well written and comprehensive • This is its main strength and its main weakness • It is incredibly inclusive and this means very little is emphasised and very little is prioritised
The strategy as a viable document: the reader’s role of interpretation • The strategy demands a major and active role of interpretation: it includes everything (in footnotes) and delivers nothing • The role of interpretation is dangerous in terms of implementation (competing viewpoints all equally correct: potentially problematic with cross disciplinary work) • The sensitivity of some points seems to have led to them being deliberately introduced through the back door (in footnotes and references)
The strategy as a viable document: interpretation and joint work • Joint work relying on interpretation is problematic and will prevent implementation and action • People will retain the status quo and not address the innovative attempt to influence the cultural and social factors which impact upon sexual well being
Cultural, social vs individual issues: the issue of prioritisation • The strategy presents an inclusive, all encompassing, focus upon all individuals and their sexual health and well-being • Every individual can see their own sexual health and well being written into the strategy
Cultural, social vs individual issues: the issue of prioritisation • The strategy states that sexual ill health can affect anyone throughout their life and that it is important to recognise that sexual well-being is an issue for all of society. • In the penultimate section (6.1), it states that ‘even more importantly, individuals have a responsibility for managing their own sexual health and maximising their sexual well-being’
Cultural, social vs individual issues: the issue of prioritisation • This levelling and sharing of sexual ill health across the population is both welcome and dangerous. • Implicitly, it suggests there is equality in access to sexual well-being, that we all face the same barriers, opportunities and service requirements. This clearly is not true.
Cultural, social vs individual issues: the issue of prioritisation • The issue of targeting, prioritisation and emphasis is dealt with most directly in section 4. • Yet it fails to deliver any clear understanding of why the groups of people are listed.
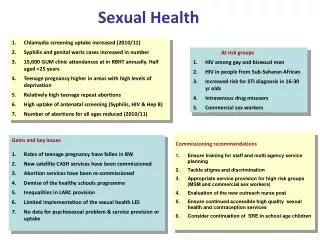
Cultural, social vs individual issues: the issue of prioritisation • There are gaps within the evidence base regarding prioritisation • However, the existing epidemiology clearly shows that if you are a man having sex with other men, or indeed someone who has travelled, or been born in, Sub-Saharan Africa, given the same sexual behaviour as most people in Scotland, you are significantly more likely to be involved in exposure to STIs and specifically HIV
Cultural, social vs individual issues: the issue of prioritisation • Prevalence of STIs (and HIV) and patterns of sexual mixing all dictate the likelihood of sexual behaviour impacting upon sexual health. • People living with HIV, or indeed Hep B, are a clear priority group in terms of promoting positive sexual health as they are involved in every new infection.
Cultural, social vs individual issues: the issue of prioritisation • There are clear inequalities in sexual health, clear socially, culturally and medically defined groups of people who consistently face far more barriers to sexual well-being than the average person in Scotland. • These inequalities must be addressed clearly in the shape of the prioritisation of certain groups (e.g. based on incidence, prevalence, health economics).
Cultural, social vs individual issues: the issue of prioritisation • The strategy reflects various social institutions such as the family (parents and carers), the school and the role of reproductive services. • Given the acknowledgement of social and cultural factors it seems strange not to explicitly highlight the role of community. • It seems as if an individualistic model of health is implicit here and that ideas of community, which often shape sexual mixing and sexual conduct, are not fully addressed and utilised in terms of promoting sexual well-being. (e.g. gay, BME, faith and geographic communities)
The cultural and social vs public health perspectives • Given the importance of social and cultural influences upon sexual health, the strategy seems to shift emphasis towards a public health (and more medical) perspective from section 4.1. onwards • In terms of the recommendations following 4.49, we see that ‘HIV testing should be made in the context of the HIV test being presented as a routine recommended test’.
The cultural and social vs public health perspectives • Given the stigma, social and sexual exclusion experienced by many positive people following HIV diagnosis I am concerned about the ‘routine’ description of the HIV antibody test (Flowers, Duncan and Frankis, 1998; Flowers et al 2003) • Given the strategies emphasis upon the social and cultural I think this recommendation is giving out the wrong message: a solely medical one • Research shows that the HIV antibody test is never routine and that appropriate pre- and post- test counselling should always be offered • Such discussions should be entrenched within the social and cultural issues surrounding HIV status (namely the legal context, community expectations of status disclosure, assumptions of status and negotiating sex). (Flowers et al., 1999)
Absences in the strategy • The central role of stigma, shame and guilt associated by many with acquiring STIs seems surprisingly absent from much of the strategy (could be included in page 15-17). • In reducing stigma and promoting sexual health check ups many of the barriers to sexual well-being could be reduced (its mentioned on page 17). Decreased delay would reduce new infections. • Overall the strategy does not address the untapped expertise of people who have acquired, are privileged by, or indeed have learnt the skills required for sexual well-being. These people offer a great resource for everyone and an opportunity for skills transfer. Also taps in to lack of evidence on this subject.
Absences in the strategy • National audit/library of resources (tier one), reducing inconsistencies, duplications • National monitoring of agencies, in terms of remit, output, effectiveness (allowing interagency comparisons and highlighting examples of good practice) • Under-representation of women’s sexual dysfunction (e.g. inoragsmia, vaginismus). Sexual dysfunction seems very male oriented.
Absences in the strategy • Targets and priorities should be set to ensure strategic direction and guide implementation • Outcomes could be based upon the social and cultural model of sexual well-being (not simply medical or public health) • E.g. Made an informed decision around HIV testing Lack of regret at first sexual encounter Celibacy as a positive choice Promotion of better masturbation techniques Reciprocal pleasure in sex with regular partner
Absences in the strategy: the crisis in gay men’s HIV prevention • The crisis in gay men’s HIV prevention is not mentioned (rising UAI, rising resistant strains of HIV) • Increases in UAI amongst gay men in Australia (Van de Ven, Rawstorne, Crawford and Kippax, 2002) in USA (Ekstrand, Stall, Paul, Osmond and Coates, 1999), in UK (Dodds, Nardone, Mercey and Johnson's, 2000; Elford, Bolding and Sherr, 2002; Rani, Woolley and Chandiok, 2000; Williamson and Hart, 2003) • In Scotland, Williamson and Hart (2003) reported that UAI increased from 32% to 34% and 43% across the three years. • The reported increase in figures for UAI with casual partners from 10.7% to 11.2% and sharper increase to 18.6% in 2002
Absences in the strategy: the medicalisation of HIV care • The medicalisation of HIV care seems absent although there is a worrying suggestion that agencies for people living with HIV should expand to a broader remit of STIs. • While the number of positive people in medical care grows, consultation times within clinics shrink and there is an increasingly narrow focus of care. Adherence, side-effects, Multi-drug resistant virus • The needs of HIV positive people have increased and not decreased
Conclusion • I think that the strategy is incredibly refreshing and positive in terms of its general ethos. • It represents a welcome move away from a medical model of sexual health towards embracing the social and cultural determinants of sexual health. • However, as it stands, it does not present a clear framework of priorities and strategic direction. • It comprehensive coverage of many key areas puts them on the agenda but may lead to confusion and disarray in terms of the process of implementation.