Download
1 / 1
10 likes | 82 Views
Learn about a case of severe obstructive hydrocephalus due to a brain tumor, requiring emergent intervention. Discover the patient's journey from diagnosis to treatment, highlighting the importance of early recognition and neurosurgical intervention.

E N D
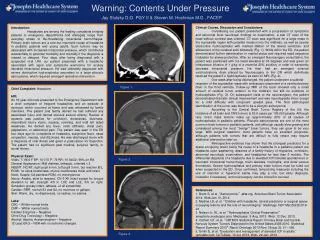
Warning: Contents Under Pressure Jay Slutsky D.O. PGY II & Steven M. Hochman M.D., FACEP Introduction: Headaches are among the leading complaints bringing patients to emergency departments and etiologies range from everyday stress to life-threatening intracranial hemorrhages. Primary brain tumors are a rare but important cause of headache in pediatric patients and young adults. Such tumors may be associated with increased intracranial pressure, which contributes substantially to potential morbidity and mortality if the diagnosis is missed or delayed. Four days after being diagnosed with a suspected viral URI, our patient presented with a headache associated with signs and symptoms worrisome for acutely elevated intracranial pressure. He was ultimately diagnosed with severe obstructive hydrocephalus secondary to a large pilocytic astrocytoma, which required emergent operative intervention. Clinical Course, Discussion and Conclusions: Considering our patient presented with a progression of symptoms and abnormal focal neurologic findings on examination, a stat CT scan of the head without contrast was ordered. CT scan was significant for a large mass in the suprasellar region with possible invasion into the midbrain, as well as severe obstructive hydrocephalus with marked dilation of the lateral ventricles, and effacement of the cerebral sulci bilaterally (Fig. 1). While still in the ED, the patient demonstrated further deterioration in mental status and required rapid sequence intubation for airway protection. After an emergent Neurosurgery consultation, the patient was positioned with his head elevated at 30 degrees and was given an intravenous infusion of 1 g/kg of a mannitol 20% solution, in order to transiently decrease intracranial pressure. He then had an emergent external ventriculostomy drain placed by Neurosurgery in the OR which definitively resolved the patient’s hydrocephalus as seen on MRI (Fig. 2). One week after being discharged, the patient underwent a subtotal resection of the suprasellar mass with endoscopic placement of a ventriculostomy drain in the third ventricle. Follow-up MRI of the brain showed only a small amount of residual tumor anterior to the midbrain, but still no evidence of hydrocephalus (Fig. 3). On subsequent visits to the neurosurgeon, the patient demonstrated dramatic clinical improvement and was neurologically intact except for a mild difficulty with congruent upward gaze. The final pathological identification of the tumor was found to be a pilocytic astrocytoma. According to the Central Brain Tumor Registry of the US, the incidence of all brain and CNS tumors is 20.6 cases per 100,000 people. Although rare, brain mass lesions make up approximately 20% of all causes of hydrocephalus in pediatric patients. Pilocytic astrocytomas are one of the most common brain tumors in pediatric patients, and although usually slow-growing and considered among the most “benign” brain tumors, they can grow to be very large. With surgical resection, most patients have an excellent prognosis, although patients with tumors that are difficult to fully resect may require additional intervention later on. Retrospective evidence has shown that the strongest predictors for a space-occupying lesion being the cause of a headache in a pediatric patient are headache upon awakening, absence of a family history of migraines, confusion, abnormal neurologic examination, and headaches for less than 6 months. The differential diagnosis of a headache due to elevated ICP includes spontaneous or traumatic intracranial hemorrhage, brain abscess, meningitis, and dural venous thrombosis. Severe hydrocephalus and primary brain tumors must be ruled out when suspected in the ED. Once confirmed, temporizing measures including the use of mannitol or hypertonic saline may play a role, but early diagnosis, intubation if necessary, and neurosurgery can be critical for survival. Figure 1. Chief Complaint: Headache HPI: An 18-year-old male presented to the Emergency Department with a chief complaint of frequent headaches and an episode of syncope, which occurred at home and was witnessed by family members. The patient and family denied he had suffered any associated injury and denied obvious seizure activity. Review of systems was positive for confusion, drowsiness, dizziness, intermittent blurry vision, nausea, vomiting, and mild left sided weakness. He denied any fever, neck stiffness, chest pain, palpitations, or abdominal pain. The patient was seen in the ED four days ago for complaints of headache, subjective fever, nasal congestion, nausea, and dizziness. He was discharged home with a diagnosis of viral illness and given a prescription for ibuprofen. The patient had no significant past medical, surgical, family, or social history. Physical Exam: Vitals: T: 98.6 F BP: 101/70 P: 79 RR: 16 SaO2: 99% on RA General Appearance: Mild distress, lethargic, oriented x 3 HEENT: NC/AT, right pupil 6 mm, left pupil 3 mm, but reactive B/L, EOMI, no sinus tenderness, mucus membranes moist and intact Neck: Supple, full painless ROM, no meningismus Neuro: Awake, slow to respond, CN II-XII intact except for tongue deviation to left, strength 4/5 in LUE and LLE, 5/5 on right. Sensation grossly intact, reflexes +2 all extremities Cardiac: RRR, normal S1 and S2, no murmurs or gallops Skin: Warm, dry, no diaphoresis, no rashes, no edema Labs: CBC – Within normal limits CMP – Within normal limits Cardiac Enzymes – Negative Urine Drug Toxicology – Negative Alcohol, Aspirin, Acetaminophen – Negative 12-Lead EKG – NSR with no ischemic changes Figure 2. References: Brem S, et al. “Astrocytoma.”abta.org. American Brain Tumor Association 2014. Web Jan 10, 2014 Medina LS, et al. “Children with headache: clinical predictors or surgical space-occupying lesions and the role of neuroimaging”Radiology 1997 Mar;202(3):819-24 Nelson Jr. SL, et al. “Hydrocephalus Clinical Presentation”emedicine.medscape.com. Medscape. 5 Aug. 2013. Web. 12 Dec. 2013. Ostrom QT, et al. “CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States 2006-2010. Statistical Report Summary 2013”Neuro-Oncology 2013 Nov; 15(sup 2): ii1 – ii56. Smith E, et al. “Evaluation and management of elevated ICP in adults.” uptodate.com. UpToDate. 10 Jul. 2013. Web. 22 Jan. 2014 Figure 3.