Download
1 / 47
470 likes | 623 Views
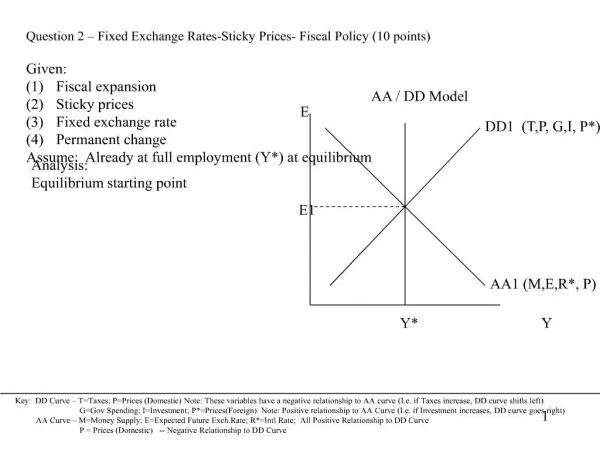
AA Development. Chapter 23 (cont): HIV/AIDS Apr 22, 2009 Class #38. Acquired Immune Deficiency Syndrome. AIDS. Acquired immune deficiency syndrome New and infectious Worldwide, the majority of HIV+ are heterosexual non-drug users.

E N D
AA Development Chapter 23 (cont): HIV/AIDS Apr 22, 2009 Class #38
AIDS • Acquired immune deficiency syndrome • New and infectious • Worldwide, the majority of HIV+ are heterosexual non-drug users. • HIV – human immunodeficiency virus (attacks the immune system, notably the helper T cells and macrophages). • HIV+ can be asymptomatic for years.
First AIDS Patients • 1980: • 55 young men diagnosed with cluster of similar symptoms of unknown origin • Gaetan Dugas (“Patient Zero”) • Bragged about having 2500+ sexual partners • 250 per year
First AIDS Patients • Symptoms looked like Kaposi’s sarcoma • Rare cancer found only among elderly • 1984: New virus isolated • All white gay males • Shortly afterwards other ethnic groups • 1991: 100,000th victim • 1993: 200,000th victim • 1994: 400,000th victim • Increased incidence of women and no effective drug treatments • 2006: 25 million deaths (65 million infected)
Demographics • Center for Disease Control and Prevention (2004) • 82% of those living with AIDS in US were males • 73% between 25-44 • Only 1% 14 or under • Misleading # because of incubation period
Demographics • Gender • Since, 1985 AIDS cases among women in US has more than tripled • 47.3% are womenHIV and AIDS increasing more rapidly in women than any other group of people
Reasons for the Increase in Women • More of virus found in ejaculations than in vaginal fluids • Also much easier washed off of penis than vagina • Therefore, male-to-female transmission of HIV is far more common than female-to-male transmission
Reasons for the Increase in Women • HIV levels in women are half that of men thus they progress to AIDS faster • Less control over using condom • Subordinate to men in many cultures • Needles used in illicit drug use often used after male partner has used it leading to greater risk of infection
Ethnicity • 78% of HIV/AIDS women are African-American and Hispanic despite accounting for less than 25% of all women in US • 45% of AIDS cases of individuals who are African-American and Hispanic is caused by injection drug use • Only 17% of AIDS cases who are Caucasian fall into this category
AIDS – Route of Transmission • Three main routes for infection – • Sexual activity involving the exchange of body fluids • Sharing contaminated needles • Birth by infected mother • Highest rates among 20-45 year olds • 2-3 times higher in men
HIV enters the bloodstream through: Open Cuts Breaks in the skin Mucous membranes Direct injection HIV Transmission
Common fluids that are a means of transmission: Blood Semen Vaginal Secretions Breast Milk HIV Transmission
HIV in Body Fluids Blood 18,000 Semen 11,000 Vaginal Fluid 7,000 Amniotic Fluid 4,000 Saliva 1 Average number of HIV particles in 1 ml of these body fluids
Routes of Transmission of HIV Sexual Contact:Male-to-male Male-to-female or vice versa Female-to-female Blood Exposure:Injecting drug use/needle sharing Occupational exposure Transfusion of blood products Perinatal:Transmission from mom to baby Breastfeeding
Blood Supply • The risk ofgetting HIV from a • blood transfusion in the U.S. is • extremely low • All blood donors are screened • for their risk of HIV • All donated blood is tested • All blood that tests positive for • signs of HIV is destroyed Source: American Red Cross HIV/AIDS Program: HIV Education and Prevention MDE HIV/AIDS PROGRAM
From HIV Infection to AIDS:Four Stages of Progression • Introduction of the retrovirus: HIV. Incorporated into the genetic material of a cell. Gradual decrease in T4 (CD4), helper t-cells over many years… • 4 Stages: • Stage 1: Immune System destroys most HIV • Mild symptoms like those of other diseases (e.g., soar throat, fever, rash, headache). Lasts 1-8 weeks. • Stage 2: Latent period for as long as 10 years or more with no or few symptoms • T cell concentration falls dramatically during this time; HIV constantly replicated • Within five years, 30% will move on to Stage 3
From HIV Infection to AIDS:Four Stages of Progression • Stage 3: AIDS related complex • T cells further reduced • Immune function impaired • Opportunistic infections occur • Kaposi’s sarcoma • Cluster of symptoms • (e.g., swollen glands, loss of appetite, fever, fatigue, night sweats, persistent diarrhea) • Stage 4: Severe immune impairment • Almost all natural immunity is lost • T cell levels drop below 100 (1000 is considered healthy level) • Multiple opportunist infections (e.g., lungs, gastrointestinal tract)
From HIV Infection to AIDS Schematic of T cellbeing attacked by HIV virus
AIDS Diagnosis • “AIDS” diagnosis after development of: • Kaposi’s sarcoma, pneumocystis carinii pneumonia, or very low levels of CD4. • Viral load test: determines level of HIV in body. • Damage to part of the immune system that fights viral infections – existing antibodies usually still work • HIV attaches to CD4 and replicates itself, destroying the cells function
Prognosis • Unfortunately, HIV/AIDS diagnosis is still a “death sentence” • Not one well-documented case of infected person whose immune system has been completely cleared of the virus
Preventive Vaccine??? • Biomedical researchers are looking for a vaccine to minimize and control the impact of HIV on the body • Major problems: • In an infected person, an estimated 10 billion new viruses are made every day • New strains are constantly appearing • Rapid speed that virus decreases T cells
But there is reason for hope… • Before 1995, there was really no treatment for AIDS patients • Today, an “AIDS cocktail” approach has increased hope that one day it will become a manageable chronic disease rather than a terminal disease
Treatment of AIDS/HIV • Purpose • Halt viral replication • Prevent opportunistic infections • Treat infections as the occur • Maintain physical and mental well being • Antiviral Therapy • Maximize suppression of virus • Preserve immune function • Prolong efficacy, delay resistance • Patient compliance, tolerable regimens • Preserve future treatment options
Why palliative care for people with HIV/AIDS? • Dramatic changes in HIV/AIDS care • Increasing body of knowledge and expanded definition of palliative care • Shift in the trajectory of dying from HIV/AIDS • Patients with HIV/AIDS have palliative care needs at each stage of the illness
HAART Regimen • Today’s optimum treatment for HIV/AIDS victims • Involves multiple anti-HIV drugs that prevent the virus from replicating within host cells
HIV/AIDS: Pre-HAART era • Rapidly fatal course • Emphasis on treating opportunistic infections and on providing palliative care • Physicians and other care providers received specific training in palliative care
HIV/AIDS in the HAART era • Chronic, manageable disease for many • Unpredictable course with more prognostic uncertainty • Complex treatment regimen requiring specific expertise • Multiple symptoms with complex etiologies • Focus of care and training on HAART and not on palliative care
Definition of Palliative Care • Medical treatment to prevent, relieve, or reduce symptoms of a disease without effecting a cure • Not intended to replace disease-modifying treatments such as antiretrovirals, but to augment the comfort and support of individuals and families who are living with life-threatening illness Center for Palliative Care Education
Importance of palliative care in HIV/AIDS • HIV/AIDS still a leading cause of death among Americans ages 15-44 • Co-morbidities of Hep B & C and malignancies can be fatal • HAART is not a cure and has many side effects • Many symptoms throughout the disease impact quality of life • Complex psychosocial issues such as psychiatric illness and substance abuse
Importance of palliative care in HIV/AIDS • HIV/AIDS disproportionately impacts minority and marginalized populations • These groups often enter care later in the disease progression • Some groups have less access to HAART • Some lack the support system to adhere to a complicated medication regimen
Traditional view of Palliative Care Therapies to modify disease(curative, restorative intent) Hospice Diagnosis Death BereavementCare
AIDS (past): Trajectory of dyingSteady decline Health Status Decline Death Time Institute of Medicine
AIDS (present): Trajectory of dying Periodic crises Health Status Decline Crisis Time Institute of Medicine
The Continuum of Palliative Care Therapies to modify disease(curative, restorative intent) Life Closure Actively Dying Diagnosis Death Therapies to relieve suffering, improve quality of life BereavementCare
HIV/AIDS Palliative Care • Integrated with disease-modifying therapies • Interdisciplinary approach • Patient & family-centered • Focus on quality of life • Multidimensional focus—physical, emotional, social, spiritual • Collaboration with patient to develop care goals
How do psychological factors predict the acquisition of HIV? • Unprotected sex • ARRM – Aids Risk Reduction Model (Catania et al., 1990) Understand the threat and recognize that ones behavior may put one at increased risk • Knowledge of risks does not always relate to preventive behaviors: College students and sex – because people are like you does not mean he/she might not be HIV positive • How much control does one have over another person’s previous sexual experience? The tendency to perceive a potential sex partner as safe
How do psychological factors predict the acquisition of HIV? • Positive attitudes towards condoms tends to increase their use • The influence of drugs and alcohol use on unprotected sex.
How do psychological factors predict the progression of HIV? • Stress – might increase the onset of AIDS due to compromised immune system functioning • The use of active-coping strategies slows the rate of progression of HIV. Some research suggest that avoidance coping for some HIV positive men, slowing the rate of decline of CD4 cells (Mulder et al., 1999). • Optimism is related to increase health behaviors, the sense of control is important. • Social support is important. Persons have reduced anxiety, depression, and slower rates of HIV progression. • Regular exercise can delay progression of HIV.
Psychosocial Barriers to AIDS Intervention • Condom Use • Over 80% of college students report having engaged in sexual relations yet only one-third use condoms • Often they report feeling awkward in asking partner about its use • Depth of Relationship • Whether the relationship is an established and committed relationship is related to high HIV risky behaviors (Sheeran et al., 1999) • Major drop-off of condom use as relationship advances • Recent Medical Advances • Less fear now • Recent developments of treatments might lead to increase risky behaviors (Vanable et al., 2000)
Psychosocial Barriers to AIDS Intervention • Psychological Factors • Optimistic Bias • Invincibility Fable • Personality Type • Sensation-seeking
Mass Screening • Most state and federal programs have primary prevention programs that include HIV screening and basic counseling • Health psychologists teach individuals to use self-control in sexual relationships • Imagery • Role-Playing
Promoting Disclosure • Often HIV-positive individuals do not disclose to their partners this information • Preventative counseling by health psychologists help increase the likelihood that they will
Complications • Family members and partners may have long-term negative effects even after patient has died • High burn-out among health-care providers and caregivers working with HIV/AIDS patients
Credits • http://www2.una.edu/psychology/health/ch10%20chronic3a.ppt • http://www.healthyschoolsms.org/ohsmain/documents/HealthisAcademicHIVAIDSPrevention.ppt#273,12,Slide 12 • http://www.ndhiv.com/programs/mediafiles/HIV101.ppt#275,7,Routes of Transmission of HIV • http://depts.washington.edu/pallcare/training/powerpoints/Palliative_Care_HIVAIDS_Overview.ppt