Download
1 / 31
330 likes | 878 Views
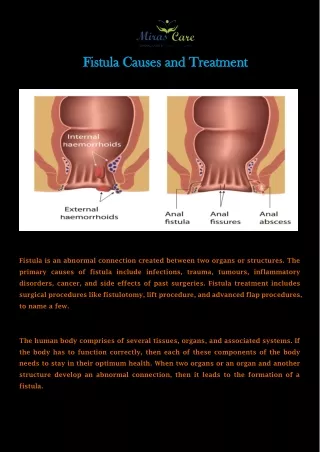
Review on enterocutaneous fistula. Definition. Enterocutaneous fistula Abnormal pathological connection between skin and GI tract Fistula output High output > 500ml / 24 hr Non high output Moderate output: 200-500ml / 24 hr Low output: <200 ml / 24 hr.

E N D
Definition • Enterocutaneous fistula • Abnormal pathological connection between skin and GI tract • Fistula output • High output • > 500ml / 24 hr • Non high output • Moderate output: 200-500ml / 24 hr • Low output: <200 ml / 24 hr Current Management of Enterocutaneous Fistula Journal of Gastrointestinal Surgery 2006;10:455–464
Causes • Post abdominal surgery • Leading cause, 75-85% • Malignancy • Infection / inflammation • IBD, diverticulitis, appendicitis, PPU, etc • Radiation • Abdominal trauma • Congenital
Prognosis • Mortality • Overall mortality 10-20% • Mortality up to 30-35% for high output fistula • Spontaneous fistula closure • ~30%, range from 20-80% • 80-90% closure within 6 weeks
Mortality sepsis Fluid and electrolyte disturbance malnutrition
Prognostic factors on fistula closure rate Reference: Nutrition and Enterocutaneous Fistulas Journal of Clinical Gastroenterology 2000;31(3):195–204
Management approach for ECF • SNAP • S: stabilization, sepsis control, skin care • N: nutrition support • A: assessment of anatomy • P: plan of definitive treatment / surgery Management of Complex Gastrointestinal Fistula Current Problems in Surgery 2009; 46: 384-430
Stabilization • Fluid and electrolyte correction • Sepsis control
Fluid and electrolyte • Aggressive monitoring and replacement of fluid, electrolytes and acid-base • Control of fistula output • Modification of enteral intake • NPO • Restriction of hypo-osmolar fluid intake / intake of fluid rich in sodium / glucose • Low residual diet / elemental diet • Pharmacotherapy • Anti-motility agents • PPI • Somatostatin / analogue
Somatostatin and its analogue • Review on randomized controlled trial on effect of somatostatin / octreotide on fistula healing Nutrition and management of enterocutaneous fistula BritishJournalofSurgery2006;93:1045–1055
Somatostatin and its analogue • Time to closure • Somatostatin may shorten time to closure • Octreotide result inconsistent • Fistula closure rate • Most studies show no significant improvement in fistula healing rate with somatostatin / octreotide
Sepsis control • Source of sepsis • Intra-abdominal collection • Others: catheter related infection, skin infection, chest infection, UTI • Assessment • CT scan • Drainage of collection • Image guided percutaneous drainage • Surgical drainage +/- proximal diversion
Skin care • Various barrier device / skin protectants • Suction drainage of fistula • VAC system for open wound • There were a few case series in which VAC was used in managing ECF with open wound successfully (Cro and colleagues, Gunn and colleague)
Skin care Current Management of Enterocutaneous Fistula Journal of Gastrointestinal Surgery 2006;10:455–464
Nutrition Nutrition and Enterocutaneous Fistulas Journal of Clinical Gastroenterology 2000;31(3):195–204
TPN • Important in management of ECF • Indicated when enteral feeding not feasible or inadequate
Enteral feeding vs bowel rest • No randomized trials investigating outcomesin patients with early enteral feeding vscomplete bowel rest have been performed • Experience from studies with aggressive approach to early enteral nutrition show similar outcome in terms of mortality and fistula closure rate compared to other studies with more parenteral nutrition
Enteral feeding • Preferred if feasible after initial stabilization • Improve mucosal integrity • Avoid complication of TPN • Access • Oral • Feeding tube / stoma distal to fistula • Fistuloclysis: tube feeding via fistula to distal limb of GI tract
Assessment of anatomy • Site of origin of fistula • Anatomy of fistula tract • Complexity • Length of tract • Defect size • Status of distant bowel • Integrity • obstruction
Assessment of anatomy • CT scan • Intra-abdominal collection • Underlying causes • Fistulogram • Anatomy of fistula tract and GI tract • Other GI contrast study • MRI • Endoscopy
Definitive plan of management • Conservative • Surgery • Novel treatment
Spontaneous closure unlikely.. • FRIEND • Foreign body • Radiation injury • Inflammatory bowel disease • Epithelialization of fistula tract • Neoplasm • Distal obstruction
Surgical intervention • Indications • Conservative management fails • Sepsis cannot be controlled • Timing of surgery • Preferably 3-6 months after presentation / previous operation unless life-threatening sepsis • Patient well optimized and disease well assessed
Surgical intervention • Surgical approach • Incision and access • Adequate mobilization / assessment of bowel • Resection vs repair • Diversion: stoma / bypass • Abdominal wall closure
Surgical intervention • Resection of diseased bowel with primary anastomosis more preferable than repair of defect if possible • Lower risk of recurrence as demonstrated in a retrospective study from Cleveland (Annals of Surgery, Volume 240, Number 5, November 2004) General rate of recurrence after surgery ranged from 10-35%
Novel treatment • Fibrin glue • A non randomized study from Mexico study on the use of fibrin glue on patients with low output fistula and showed shorter healing time compared to control group (World Journal of Gastroenterology, 2010 June 14; 16 (22): 2793 – 2800) • Gelfoam embolization • Fluoroscopic guided placement of catheter at the enteric opening of the fistula and gelfoam was injected to occlude the fistula at its enteric opening • A case series from Australia (Lisle and colleagues) reported successful use of gelfoam embolization in treating 3 patients with low output fistula (Disease of the Colon and Rectum 2006; 50: 251–256)
Fistuloclysis • A case series was reported in UK (Teubner and colleagues), in which fistuloclysis was attempted in 12 patients with small bowelfistulas, 11 out of the 12 patients were able to wean off TPN Fistuloclysis can successfully replace parenteral feeding in thenutritional support of patients with enterocutaneous fistula British Journal of Surgery 2004;91:625–631
Gelfoam embolization Percutaneous Gelfoam Embolizationof Chronic Enterocutaneous Fistulas:Report of Three Cases Disease of the Colon and Rectum 2006; 50: 251–256