Download
1 / 26
311 likes | 728 Views
Management of Acute Diarrhoea in Children. Welcome to the module on Management of Acute Diarrhoea (AD) in Children! Diarrhoea l disease remains a leadin g cause of morbidity and mortality amongst children in l ow and middle income countries.

E N D
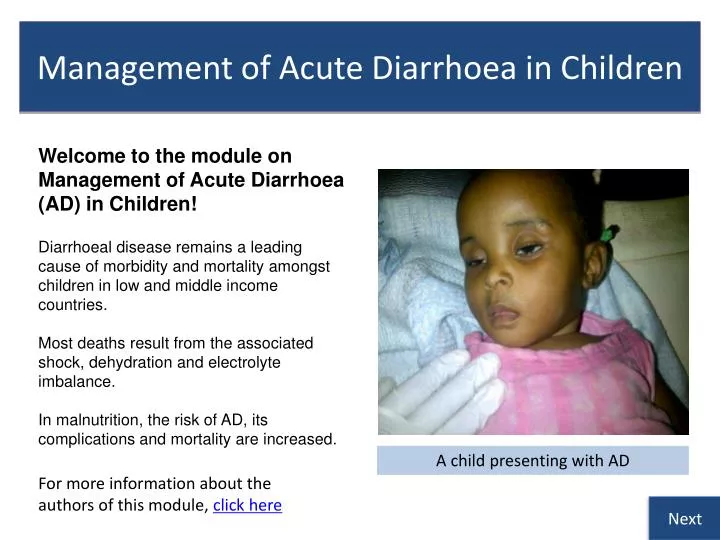
Management of Acute Diarrhoea in Children Welcome to the module on Management of Acute Diarrhoea (AD) in Children! Diarrhoeal disease remains a leading cause of morbidity and mortalityamongst children in lowand middle income countries. Most deathsresult from the associated shock, dehydrationand electrolyte imbalance. In malnutrition, the risk of AD, its complications and mortality are increased. A child presenting with AD For more information about the authors of this module, click here Next
How to use this module • This module aims to address deficiencies in the management of AD and dehydration in children that we identified during a clinical audit. • We suggest that you start with the learning objectives and try to keep these in mind as you go through the module slide by slide, in order and at your own pace. • Print-out the diarrhoea SDL answer sheet. Write your answers to the questions (Q1, Q2 etc.) on the sheet as best you can before looking at the answers. • Repeat the module until you have achieved a mark of >20 (>80%). • You should research any issues that you are unsure about. Look in your textbooks, access the on-line resources indicated at the end of the module and discuss with your peers and teachers. • Finally, enjoy your learning! We hope that this module will be enjoyable to study and complement your learning about AD from other sources. Next Click here to move to the next slide
Learning Outcomes By the end of this module, you should be competent in the management of acute diarrhoea / dehydration. In particular you should be able to: • Describe when to use oral and parenteral fluids and what solutions to use • Identify the malnourished child and adjust management accordingly • Describe when antibiotic treatment is indicated and the adverse effects of the overuse of antibiotics • Describe the use of zinc in AD Next
Definition of AD • There is a wide range of normal stool patterns in children which makesthe precise definition of AD difficult • According to the World Health Organization (WHO), AD is the passage of loose* or watery stools, three times or more in a 24 hour period for upto14 days • In the breastfed infant, the diagnosis is based on a change in usual stool frequency and consistency as reported by the mother • AD must be differentiated from persistent diarrhoea which is of >14 days durationand may begin acutely.Typically, this occurs in association with malnutrition and/orHIV infection and may be complicated by dehydration *Takes the shape of the container Diaper stained with watery stool Next
The burden of diarrhoeal disease • Despite the fact that diarrhoea can be prevented, about 2 billion cases of diarrhoea occur globally every year in children under 5 years • About 2 million child deaths occur due to diarrhoeaevery year • More than 80% of these deaths are in Africa and South Asia • Diarrhoea is the third most common cause of death (see diagram) • In Nigeria, diarrhoeacauses 151,700 deaths of children under five every year,* the second highest rate in the world after India * UNICEF/WHO, Diarrhoea: Why children are still dying and what can be done, 2009 Causes of death among children under age of five years UNICEF: Progress for children, 2007 Next
Causes and risk factors for AD • Microbial, host and environmental factors interact to cause AD • Click on the boxes to find out more Next
Clinical types of AD • There are 2 main clinical types of AD • Each is a reflection of the underlying pathology and altered physiology Next
Q1Write “T” or “F” on the answer sheet. When you have completed all 5 questions, click on each box and mark your answers. • The incidence of AD is highest in the age group 6-11 months • Acute diarrhoea is of duration less than 14 days • Rotavirus is a more common cause of diarrhoea in developing countries than bacterial pathogens • Undernutrition is a major risk factor for persistent diarrhoea • The largest proportion of deaths from diarrhoea occur in East Asia a b c d e Next
Clinical scenarios • You will now work through a series of cases of AD • You will learn how to assess and manage children according to the latest WHO guidelines • Start with scenario A. Try to answer the questions yourself before clicking on the answers http://www.who.int/maternal_child_adolescent/documents/9241546700/en/index.html Next
This 2 year old child was rushed into the emergency room. She had AD and had become very unwell. Scenario AAssessment and management of shock Q2. How would youproceed? Write down your answer before moving to the next slide! Next
This 2 year old child presented with AD. She did not have features of shock or SAM but was assessed to have severe dehydration. Scenario BClinical assessment of dehydration Q4. List the 4 clinical signs recommended for classifying a child as severely dehydrated Write down your answers and then go to the next slide Next
Scenario C Clinical assessment of dehydration A mother brought her 2 year old male child to the hospital because of AD. On examination, he was irritable and his skin pinch goes back slowly (1 second) Q8: Write down your assessment of this child’s hydration status Q9: List 2 other key clinical signs consistent with this degree of dehydration Write down your answer and then go to the next slide Next
Scenario D A child with bloody diarrhoea A child was brought to the emergency room because of bloody diarrhoea of 3 days duration with associated vomiting and fever. When examined, there were no signs of dehydration or SAM. Q11: What it is the most likely diagnosis in this child? Q12: How will you treat? Write down your answers and then move to the next slide Next
Answers: Scenario D Q11: • This child has acute bloody diarrhoea also called dysentery • Most episodes are due to Shigella spp • The diagnostic signs of dysentery are frequent loose stools with visible red blood • Other findings in the history or on examination may include • Abdominal pain • Fever • Convulsions • Lethargy • Dehydration • Rectal prolapse Q12: All children with severe dysentery require antibiotic treatment for 5 days • Give an oal antibiotic to which most strains of shigella in your localiity are sensitive • Examples of antibiotics to which shigella strains can be sensitive are ciprofloxacin and other fluoroquinolones Also manage any dehydration Ensure breastfeeding is continued for childen still breastfeeding and normal diet for older childen Follow-up the child Go to Case Scenario E
Scenario E Clinical assessment of dehydration This 2 year old male child was brought to the Children’s emergency room with diarrhoea for 6 days. He had angular stomatitis, peri-anal ulceration, weighed 7.0 kg and the MUAC was 10.2 cm. His hands were cold, pulse weak and fast and skin pinch went back very slowly. However, he appeared to be fully conscious and was not lethargic. The resident doctor gave 140ml of normal saline by rapid IV infusion but his condition deteriorated. Q13: What important condition needs to be recognised in this child? Q14: Was the doctor’s management correct? Q15: List 2 pathophysiological mechanisms in this condition that affect fluid management. Next
Answer: scenario E - Fluid management in children with SAM Q13: The child has severe acute malnutrition: SAM Q14: No.Dehydration is difficult to diagnose in SAM and it is often over diagnosed. The doctor’s choice of IV normal saline, amount of fluid and rapidity of given IV fluid were all incorrect and may have caused the child’s deterioration Q15: The pathophysiological mechanisms that affect fluid management are: • Although plasma sodium may be very low, total body sodium is often increased due to • increased sodium inside cells • additional sodium in extracellular fluid if there is nutritional oedema • reduced excretion of sodium by the kidneys • Cardiac function is impaired in SAM This explains why treatment with IV fluids can result in death from sodium overload and heart failure. • The correct management is reduced sodium oral rehydration fluid (ORF; e.g. ReSoMal) given by mouth or naso-gastric tube if necessary. The volume and rate of ORF are much less for malnourished than well-nourished children (see next slide) IV fluids should be used only to treat shock in children with SAM who are also lethargic or have lost consciousness! Next
End of clinical scenarios The next few slides are on how to assess nutritional status, indications for laboratory investigations, rational use of antibiotics and usage of zinc Next
Assessment of nutritional status • Assessment of nutritional status is important in children with diarhoeal disease to identify those with severe acute malnutrition (SAM) • This is because abnormal physiological processes in SAM markedly affect the distribution of sodium and therefore directly affect clinical management • In patients with SAM, although plasma sodium may be very low, total body sodium is often increased due to: • increased sodium inside cells as a result of decrease activity of sodium pumps • additional sodium in extracellular fluid if there is nutritional oedema • reduced excretion of sodium by the kidneys A West African child with kwashiokor Next
Methods of nutritional assessment Nutritional assessment can be done by: • Looking for visible signs of severe wasting such as muscle wasting and reducedsubcutaneous fat • Looking for other signs of malnutrition: angular stomatitis, conjuctival and palmar pallor, sparse and brittle hair, hypo- and hyperpigmentationof the skin • Looking for nutritional oedema (pitting oedema of both feet) • Use of anthropometry such as Weight-for-Height z-score (WHZ; < -3.0) or Mid-Upper Arm Circumference (MUAC < 11.5cm in children aged 6-60 months) Muscle wasting and loss of subcutaneous fat in a West African child with marasmus Next
MUAC: recommended for nutritional assessment in dehydration • MUAC is widely used in community screening of malnutrition because it is easy to perform, accurate and quick • MUAC is measured using Shakir’s strip or an inelastic tape measure placed on the upper arm midway between acromion process and olecranon • Dehydration reduces weight; MUAC was less affected by dehydration than WFLz score in a recent study* • Mid-Upper Arm Circumference (MUAC): • <115mm: SAM • 110 - 124mm: Moderate Acute Malnutrition (MAM) • 125 - 135mm: risk of acute malnutrition • >135mm: child well nourished • www.motherchildnutrition.org/ *http://www.nutritionj.com/content/10/1/92 Next
Laboratory investigations AD is usually self-limiting and investigations to identify the infectious agent are not required • Indications for stool microscopy, culture and sensitivity • Blood and mucus in the stool • High fever • Suspected septicaemic illness • Diagnosis of AD is uncertain • Indications for measurement of Urea and Electrolytes • Severe dehydration or shock • Children on IV fluid • Children with severe malnutrition • Suspected cases of hypernatreamic dehydration Next
Rational use of antibiotics • Even though bacterial pathogens are the commonest cause of AD in developing countries, there should be cautious and rational use of antibiotics to discourage development of microbial resistance, avoid side effects and reduce cost • Antibiotics should be used for: • Severe invasive bacterial diarrhoea eg Shigellosis • Cholera • Girdiasis • Suspected or proven sepsis • Immunocompromised children Antibiotics are contraindicated in: • E. coli 0157: H7 because they increase the risk of Haemolytic Uraemic syndrome (HUS) • Uncomplicated salmonella enteritis because they prolong bacteria shedding Next
Zinc and diarrhoea • Zinc deficiency is common in developing countries and zinc is lost during diarrhoea • Zinc deficiency is associated with impaired electrolyte and water absorption, decreased brush border enzyme activity and impaired cellular and humoral immunity • Treatment with zinc reduces the duration and severity of AD and also reduces the frequency of further episodes during the subsequent 2-3 months • WHO recommends that children from developing countries with diarrhoea be given zinc for 10-14 days • 10mg daily for children <6 months • 20 mg daily for children >6 months Next
How can we prevent diarrhoeal disease? This involves intervention at two levels: • Primary prevention (to reduce disease transmission) • Rotavirus and measles vaccines • Handwashing with soap • Providing adequate and safe drinking water • Environmental sanitation • Secondary prevention (to reduce disease severity) • Promote breastfeeding • Vitamin A supplementation • Treatment of episodes of AD with zinc Next
End of module • Well done! You have completed this module • Make sure that you repeat the module until you have a good score in the assessment • It is vital that you now apply the knowledge you have gained from this module into your management of children with AD • Please do let us know if you think that there are any ways that this module could be changed as a learning resource that is effective in improving practice • Please e-mail any comments to Dr. Senbanjo at senbanjo001@yahoo.com Authors and acknowledgements
Authors/Acknowledgement Authors: Dr. Idowu Senbanjo, Lecturer/Consultant Paediatrician, Department of Paediatrics and Child Health, Lagos State University College of Medicine, Ikeja, Lagos, Nigeria. Dr. Chinlye Ch‘ng, Consultant Gastroenterologist/Hepatologist, Abertawe Bro Morgannwg University Health Board, Singleton Hospital, Swansea, UK. Prof. Steve Allen, Professor of Paediatrics and International Health, RCPCH International Officer and David Baum Fellow, The College of Medicine, Swansea University, UK. Acknowledgement We would like to acknowledge the British Society of Gastroenterology for awarding an educational grant which supported Dr. Senbanjo in developing this module. Permissions Please note that consent was obtained from parents/carers to use the images in this module for teaching purposes only. The images should not be used for any other purpose. We are very interested to receive feedback regarding any aspect of this module, especially if it helps us to improve it as a learning resource. Please e-mail any comments to Dr. Senbanjo at senbanjo001@yahoo.com Back