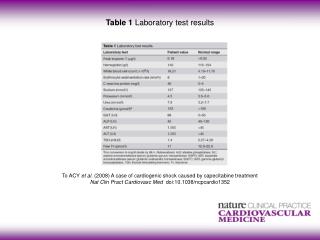
Laboratory Test Results
Laboratory Test Results. Brenda C. Barnes, MSEd , MT(ASCP)SBB and Shawn Froelich, MLS(ASCP) CM. Objectives. Correlate urinalysis reagent strip results with microscopic test results. Correlate microscopic evaluation results of a vaginal swab with clinical symptoms.

Laboratory Test Results
E N D
Presentation Transcript
Laboratory Test Results Brenda C. Barnes, MSEd, MT(ASCP)SBB and Shawn Froelich, MLS(ASCP)CM
Objectives • Correlate urinalysis reagent strip results with microscopic test results. • Correlate microscopic evaluation results of a vaginal swab with clinical symptoms. • Discuss proper collection procedures for anaerobic cultures. • Interpret microbiology susceptibility reports. • Explain the procedure for microscopic examination of skin scrapings. • Describe rapid testing available that is applicable to the clinical setting.
Chemical Exam – Glucose • Presence of glucose indicates the amount blood glucose has exceeded tubular reabsorptive capacity • Clinical correlation • Diabetes mellitus • Pancreatitis • Hyperthroidism • Gestational diabetes
Glucose • Clinitest • Nonspecific test for reducing substances • If performed, done so on pediatric specimens (< 2 years old) • Screening for galactosemia – may be part of state mandated newborn screening program • Microscopic Correlation • No elements seen • Yeast may be present
Chemical Exam – Bilirubin • Presence indicates liver disease or biliary obstruction • False-positives due to urine pigments • Ictotest – confirmatory test • Less subject to interference • False-negatives • Age of specimen – bilirubin is unstable • No microscopic correlation
Chemical Exam – Ketones • Presence indicates increased fat metabolism • Clinical significance • Diabetic acidosis • Insulin dosage monitoring • Starvation • Malabsorption • Microscopic correlation - none
Chemical Exam – Sp. Gravity • Strip reading is adequate for routine screening • Clinical significance • Monitoring patient hydration and dehydration • Loss of renal tubular concentrating ability • Diabetes insipidus • Determination of unsatisfactory specimens • Microscopic correlation – none
Chemical Exam – Blood • Presence of red blood cells, hemoglobin, or myoglobin • Hematuria - bleeding • Hemoglobinuria • Lysis of rbc in specimen • Intravascular hemolysis • Myoglobinuria – muscle destruction • Microscopic correlation – rbc seen in hematuria
Chemical Exam – pH • Of little diagnostic value – primarily used for determining systemic acid-base disorders • Microscopic correlation – none
Chemical Exam – Protein • Presence indicates abnormality in glomerular filtration barrier – renal disease • Correlates with: • Nitrite • Leukocytes • Microscopic
Chemical Exam - Urobilinogen • Increased in any condition that causes an increase in production or retention of bilirubin • Clinical significance • Early detection of liver disease • Lever disorders, hepatitis, cirrhosis, carcinoma • Hemolytic disorders • Microscopic correlation – none
Chemical Exam – Nitrite • Rapid screening for UTI • Sample needs to be fresh to avoid false-positive reactions • Correlates with: • Protein • Leukocytes • Microscopic
Chemical Exam – Leukocytes • Screening test for presence of wbc in urine • Quantification should be done by microscopic examination • Correlates with: • Protein • Nitrite • Microscopic
Microscopic Examination • Detect and identify insoluble materials present in urine • Time-consuming = cost • Lacks standardization Protocols used by many labs to improve standardization and cost-effectiveness
Vaginitis • Occurs when the mucosal lining of the vagina becomes inflamed and irritated • Typical signs: • Vaginal discharge • Vulvar itching irritation • Odor • Commonly associated diseases: • Bacterial vaginosis • Trichomoniasis • Candidiasis
Laboratory Diagnosis • Vaginal pH • KOH Amine “Whiff” test • Vaginal microscopy (wet mount) • Kit testing • BD Affirm VPIII • QuickVue Advance pH and Amines test • QuickVue Advance G. vaginalis test • OSOM® Trichomonas Rapid Test
Sample Collection • Swab vaginal vault and walls with one or two swabs • Include any areas where fluid has pooled • Place swab(s) in test tube containing 0.5 mL saline • Sample should remain at room temperature and tested within two hours of collection • Note that T. vaginalis loses viability quickly http://www.acponline.org/running_practice/mle/wm_exams.htm
Vaginal pH • Typical vaginal pH = 4.0-4.5 • > 4.5 • BV • Trichomoniasis • Tested at time of collection
Wet Mount • Vigorously mix swab(s) in and out of saline – collect all material adhering to side of tube • Remove swab from saline and depress onto clean, dry microscope slide – express small amount of fluid • Coverslip and examine under microscope http://www.acponline.org/running_practice/mle/wm_exams.htm
KOH “Whiff” Test • Prepare wet mount slide as directed, adding one drop of 10% KOH to slide prior to coverslipping • Positive test demonstrates typical “fishy” odor
Alternative Testing http://www.quidel.com/products/product_detail.php?prod=98&group=1
Bacterial Vaginosis • Presence of clue cells • Lack of visible lactobacilli • Lack of WBC • pH >4.5 • Positive “whiff” test • Demonstration of at least three of these conditions is diagnostic Mahon, 2011
Other Methods • Affirm VPIII (Becton Dickinson) • Detects G. vaginalis, Candida spp., and Trichomonasvaginalis • Some technical expertise is required • Additional equipment • Sensitivity comparable to culture http://www.bd.com/ds/productCenter/MD-AffirmVPIII.asp
Trichomoniasis • Visualization of motile trichomonads in a wet mount • Limited sensitivity – 60-70% • Need for immediate testing (within 10 minutes of collection)
Trichomonas – wet mount http://bmtjournal.blogspot.com/2007/12/mmic-case-6.html
Trichomonas – phase contrast Mahon, 2011
Trichomonas – phase contrast http://depts.washington.edu/nnptc/online_training/std_handbook/gallery/pages/trichomonasvaginalis.html
Other Methods • OSOM® Trichomonas Rapid Test • 80% sensitivity compared to culture (Mahon, 2011) • 95% agreement with culture and wet mount (product literature) http://www.sekisuidiagnostics.com/prod/poc/diag_p-OSOM-Trichomonas-Rapid-Test.asp
Candidiasis • Demonstration of budding yeast forms • pH = approximately normal http://commons.wikimedia.org/wiki/File:Candida_wet_mount.jpg
Yeast with hyphae http://depts.washington.edu/nnptc/online_training/std_handbook
Anaerobic Specimens • Most anaerobic infections are caused by endogenous microbiota • Improper collection may result in the growth of many anaerobes, resulting in difficulty to determine the cause of infection • Labs follow criteria for rejection of inappropriately collected and/or transported specimens
Acceptable Specimens for Anaerobic Culture • Aspirated material • CSF, blood, bone marrow, synovial fluid • Aspiration of closed abscess, ascites fluid, peritoneal fluid • Deep tissue or bone biopsy • Aspirated pus from decubitus ulcers • Suprapubic bladder aspiration • Pleural fluid obtained by thoracentesis, open lung biopsy, “sulfur granules” from draining fistula
Unacceptable Specimens for Anaerobic Culture • Swabs • Throat, nasopharyngeal, gingival, rectal, vaginal, cervical, urethral, surface wounds and abscesses • Expectorated or suctioned sputum, bronchial washings • Contents of large bowel, feces, colostomy effluents, gastric and small bowel contents • Voided or catheterized urine
Transport and Processing of Anaerobic Specimens • Transport and processing should be quick to maintain temperature, avoid exposure to oxygen and avoid dessication • Oxygen-free transport tubes/vials such as PRAS media (prereduced, anaerobically sterilized) • Anaerobic bags or pouches if delays in transport • Blood cultures require aseptic collection with bactericidal agent such as tincture of iodine or chlorhexidinegluconate with 70% alcohol to minimize contamination with normal skin biota
Information • Use • Identify fungal infections of the skin, mouth, and nails • Indications • Areas of broken hair or baldness • Presence of scaly lesion on skin • Crumbling or scaly nails or nail beds • White plaque in the mouth http://www.acponline.org/running_practice/mle/wm_exams.htm
Procedure • Add 1 drop of 10-20% KOH solution to slide • Add nail scrapings, hair, skin scales, or thin slices of tissue to drop of fluid • Apply coverslip • Gently heat slide • Allow slide to cool for ~ 15 minutes Mahon, 2011
KOH Test • KOH breaks down keratin and skin layers • Makes fungi more visible, if present • Additional information • Addition of dimethyl sulfoxide (DMSO) removes need for heating • Addition of stain makes fungal elements readily visible
Dermatophyte in skin scraping http://missinglink.ucsf.edu/lm/DermatologyGlossary/potassium_hydroxide_preparation.html