Download
1 / 34
340 likes | 556 Views
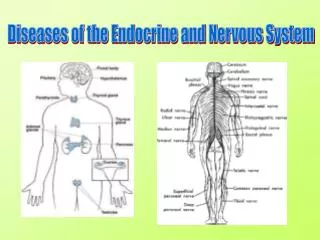
Diseases of the Nervous System. Systemic Lupus Erythematosus. Autoimmune disease that can effect nearly every system More common in women than men Symptoms can be vague

E N D
Systemic Lupus Erythematosus • Autoimmune disease that can effect nearly every system • More common in women than men • Symptoms can be vague • Butterfly rash, sun sensitivity, arthritis, serositis (inflammation of lining of lung or heart), kidney disorder, neurologic disorder • Occurs in “flares” • Organ threatening (decrease lifespan) vs non-organ threatening (normal lifespan) • top causes of death: kidney disease, infections, CNS lupus, blood clots, cardiovascular complication • Treatments • Antimalarial drugs and corticosteroids (anti-inflammatory) • Chemotherapeutic agents (immunosuppressant and inhibit cell proliferation)
Depression • Low levels of norepinephrine and serotonin in the CNS • Patients’ brains often up-regulate NT receptors in response to low levels of NT • Treatments • Monoamine oxidase inhibitors (MAOI)= higher levels of NT in the synaptic cleft or block NT reuptake by presynaptic neuron; cause high bp • Selective serotonin reuptake inhibitors (SSRI)= inhibit reuptake of serotonin by the presynaptic neuron; less side effects than MAOIs
Bipolar disorder • Periods of depression followed by periods of euphoria • Usually strikes young (~20 yrs old) and episodes recur throughout life • Treatments • Lithium= stabilizes levels of monoamines • Antidepressants for depressive attacks and antipsychotics for psychotic attacks • Anticonvulsants= control sensitivity of neural membranes to stimulatory signals
Schizophrenia • Disorganized thinking and speech, delusions, hallucinations • Onset usually between 25-35 • Excess neurotransmission by dopamine-producting neurons • Treatments • Drugs that inhibit dopaminergic neurotransmission
Parkinson’s disease • Loss of dopamine-producing neurons in a specific region of the basal ganglia • Interferes with initiation of movement • Link between this disease and people who are known for their “straight arrow” personality • Treatments • L-dopa= precursor to dopamine that crosses BBB; side effect is schizophrenia-like behavior • Dopamine agonists= bind to and activate dopamine receptors; side effect is triggering thrill-seeking behaviors
Curare poisoning • Antagonist for Ach receptors (non-depolarizing) • Blocks muscle contraction • Does not cross BBB • Death from respiratory muscle failure • Treatments • Neostigmine= drug that inhibits acetylcholinesterase so that more Ach competes for receptor binding
Myasthenia gravis • Autoimmune disease; B cells make antibodies that bind to and block Ach receptors of the neuromuscular junction • Neuromuscular disorder characterized by progressive muscular weakness and, if untreated, respiratory muscle failure • Treatments • Mechanical ventilation • Neostigmine and related drugs • Thymectomy (removal of the thymus); thymus is involved in tolerance and thymic abnormality is associated with this disease
Multiple sclerosis • Appears to be an autoimmune disease characterized by demyelination of neurons in CNS • Symptoms include blurred or double vision, muscle weakness, loss of balance, spasticity, muscle fatigue, mild cognitive impairments • Patterns: relapsing-remitting, primary progressive, or benign • Rarely fatal • ~twice as common in women than men, but men have more rapidly progressing disease • ~twice as common in people of European ancestry • Treatments • Anti-inflammatory agents such as corticosteroids • Interferon beta slows progression
Amyotrophic Lateral Sclerosis • Loss of motor neurons, both lower and upper • Pathogenesis not well understood, but may involve glutamate toxicity • ↑glutamate prolonged opening of Ca2+ channels Ca2+ activated proteases cellular damage • Symptoms include muscle weakness and cramping, muscle atrophy, loss of muscle control involved in respiration, inability to coordinate swallowing • Patterns: lower motor neurons first= asymmetric weakening of one of the limbs, upper motor neurons first= difficulty moving face and tongue • Most patients die within ~5 yrs • More common in men than women • Treatments • Riluzole= inhibits release of glutamate from presynaptic neurons • Baclofen= muscle relaxant that relieves muscle spasticity
Peripheral neuropathy • Death of peripheral nerves • Can occur as a result of a number of disorders (renal failure, alcoholism, diabetes, vitamin B12 deficiency, lead poisoning, lupus) • Symptoms: • sensory= loss of sensation in extremities • motor= weakness of skeletal muscles • autonomic= orthostatic hypotension and impaired GI function, thermoregulation, vision, & sexual function
Guillain-Barre syndrome • Autoimmune attack on myelin in peripheral nerves (as opposed to MS) • Often occurs after viral infection, sudden disease onset • Many cases are mild, but some require mechanical ventilation • ~1/2 of patients fully recover within 1 year
Spinal cord injuries • Death of nerve cells generally leads to permanent loss of function • Trauma or glutamate exotoxicity can cause cell death of neurons • Degree of disability is related to region of spinal cord injury • Injury of cervical nerves= quadriplegia • Injury of thoracic nerves= paraplegia • Injury to lumbar or sacral region= some loss of sensation and motor control in legs and hips • Treatments • Relief of compression (by traction or surgery) • Methylprednisone= corticosteriod that stabilizes cell membranes and reduces inflammation, within 8 hrs of injury
Autonomic dysreflexia • Abnormal activation of the sympathetic nervous system • Major concern for people with spinal cord injuries • Triggered by painful or irritating stimuli (full bladder, UTI, pressure wounds, GI conditions, menstrual cramps, labor & delivery) • Nerve signals get blocked at injury and do not reach brain triggers reflexes in SNS • Most dangerous effect is sudden vasoconstriction sharp rise in bp seizure, stroke, or death
Organophosphates • Active ingredient in nerve gas and many pesticides • Inhibit acetylcholinesterase • Effect on autonomic function: • ↑ parasympathetic system ↑ GI function, ↑ respiratory secretions, ↓ HR • Effect on muscle: • Depolarizing paralysis of skeletal muscle • Effect on CNS: • Triggers convulsions
Botulinum toxin • Comes from bacteria • Most toxic substance known to man • Cleaves docking proteins off of Ach-containing vesicles prevents release of Ach at neuromuscular junction and in autonomic NS • Symptoms: dry mouth, double vision, symmetric flaccid paralysis, difficulty swallowing & speaking, paralysis of respiratory muscles • Treatments • Respirator for several weeks
Strychnine poisoning • Antagonist to glycine receptors (glycine is an inhibitory NT that acts on lower motor neurons) • Lower motor neurons fire inappropriately muscle spasms throughout body severe pain • Treatments • Valium= controls muscle spasms • Must be monitored for rhadomyolysis • release of toxic levels of myoglobin from damaged muscle cells nephrotoxic
Stroke • Ischemic stroke= portion of the blood flow to the brain is blocked • Occurs when thrombus or embolus obstructs blood flow • ~ 85% of strokes • Intracranial hemorrhage= rupture of blood vessel in brain • Often result from congenital anatomical abnormalities, ~25% are fatal • ~15% of strokes • Mechanism of cell death: ↓glucose & oxygen ↓ATP loss of ion gradients anoxic depolarization release of high levels of glutamate • Treatments • Ischemic strokes treated with thrombolytic drugs= break down blood clots; administer within 3 hrs • Hemorrhagic strokes treated with surgery or clotting agents • Drugs to block glutamate and its toxic effects
hypothalamus anterior pituitary thyroid From class notes 10/23/06 (S.Shore)
Iodine deficiency • Non-toxic goiter • Leading cause of brain damage worldwide, even mild cases reduce IQ • Esp. problematic for pregnant women due to requirements of the fetus • Universal Salt Iodization adopted by WHO in 1993 • Diagnosis: goiter, increased TSH levels • Mechanism: ↓ iodine inability of thyroid to make T3/T4 ↓ serum T3/T4 less T3/T4 inhibition of anterior pituitary TSH synthesis & less inhibition of hypothalamus to turn off TRH ↑ serum TSH & ↑ serum TRH ↑ thyroid growth (goiter) increased efficiency of T3/T4 production
Hyperthyroidism • Excessive thyroid hormone • Ex: Grave’s disease= autoimmune disease • Auto-antibodies stimulate TSH receptor independent of TSH • ↑ T3/T4 negatively feeds back on anterior pituitary to ↓ TSH & on hypothalamus to ↓ TRH • Symptoms: hypermetabolism, increased sympathetic activity (T3/T4 increase expression of b-adrenergic receptors), psychological effects, overactivity of muscles retracting eyelids • Treatments: • Surgery to destroy thyroid gland (need to replace T3/T4) • Drugs to block T3/T4 synthesis • Lithium= inhibits T3/T4 secretion
Hypothyroidism • Primarily due to destruction of thyroid gland • Ex: Hasimoto’s thyroiditis= autoimmune destruction, blocks TSH receptor (as opposed to Grave’s disease that stimulates receptor) • Secondarily due to deficiency of TSH • Symptoms: vary with age at onset • Juvenile/adult: hypothermia, fatigue, decreased cardiac output, intellectual slowness, decrease sweating, weight gain, edema, etc. • Childhood: cretinism (severe mental and growth retardation) • Treatments • Administration of T3/T4
exercise stress fasting low plasma glucose sleep + - - hypothalamus SS GHRH - + - Anterior pituitary GH Liver and other cells IGF-1 From class notes 10/23/06 (S.Shore)
Acromegaly • Caused by increased growth hormone secretion • Tumor of anterior pituitary that secretes GH • Oral glucose challenge: large dose of glucose normally shuts off GH secretion, but not in acromegaly • Hypothalamic abnormality that ↑ GH secretion • Extrapituitary neoplasm that secretes GHRH • Symptoms: ↑ bone (wider) & muscle & connective tissue growth, enlargement of hands and feet, facial feature changes (coarsens features), ↑ diabetes, ↑ heart mass congestive heart failure • Treatments • Surgery to remove tumor • Analogue of somatostatin (negative regulator of GH secretion by anterior pituitary) • GH receptor antagonist
Gigantism • Etiologically identical to acromegaly • Occurs before epiphiseal plates close, allowing long bone growth in addition to wide bone growth • Results in excessive height
Dwarfism • Proportionately reduced size and stature • Caused by insufficient GH secretion or action • Treatments • Administration of human recombinant GH • Achondroplasia: genetic disease caused by mutation in FGF (fibroblast growth factor) receptor • Disproportionate: small stature & limbs with enlarged head size
From: Pathophysiology of Disease, McPhee et al. Appleton and Lange, Norwalk, CT
Diabetes Mellitus (Types I & II) From class notes on October 30, 2006 (S.Shore)
Pathogenesis of Type I • Autoimmune destruction of b-cells of pancreas • May be triggered by viral infection • Genetic component= linked to MHC II genes • Onset is usually during adolescence • Effect is not observed until >70% of b-cells are lost
Pathogenesis of Type II • Due primarily to insulin resistance • Initially leads to increase insulin secretion, but eventually b-cells can deplete and cause reduced insulin secretion • Obesity and chronic inflammation may contribute to insulin resistance • Strong genetic tendency • Strong correlation with obesity
Acute Complications of Types I & II • Hyperglycemia • Loss of glucose in urine loss of water hypotension • Increased plasma osmolarity water leaves the tissues coma (if severe) • Ketosis= lack of insulin ↑ lypolysis ↑ ketone synthesis ↓ plasma pH (more acidic) metabolic complications • Especially bad for brain! • Hyperkalemia= ↑ plasma K+ due to lack of insulin and increased plasma glucose changes in cell membrane potential (depolarizing) cardiac arrhythmias • Treatment: replacement of water, electrolytes, and insulin injections • Hypoglycemia (arising from insulin overdose) • Sympathetic discharge= low glucose stimulates hypothalamus sweating, shaking, anxiety, palpitations, weakness, tremor, tachycardia • Neuroglycopenic symptoms= lack of glucose to brain confusion, irritability, headaches, weakness, abnormal behavior, lack of motor coordination, convulsion, coma • Treatment: oral or IV glucose, glucagon injection
Chronic Complications of Types I & II • Microvascular disease (caused by ↑ glycosylation of proteins or ↑ sorbitol production) • Retinopathy= blindness • Nephropathy= renal disease, requires dialysis and/or kidney transplant • Macrovascular disease (most common in type II) • Coronary artery disease • Cerebrovascular disease • Peripheral vascular disease (leading cause of death for type II diabetics) • Neuropathies (peripheral and autonomic, caused by demyelination and loss of nerve fibers) • Loss of sensation, tingling & numbness in extremities, autonomic problems (tachycardia, impotence, incontinence, GI problems) • Foot ulcers (caused by sensory neuropathy, infection, vascular disease) • Infections (caused by effects of ↑ glucose on neutrophil function, skin eruptions, vascular disease, ↑ plasma glucose)
Treatment of Types I & II • Type I • Insulin injections • Type II • Diet • Exercise • Glucophage= ↑ insulin sensitivity, ↓ glucose production • Sulfonylureas= ↑ insulin release • Insulin= in severe cases when insulin secretion is depressed • Thiazolindiones= PPARg agonists that ↓insulin resistance