Download
1 / 1
10 likes | 119 Views
Inequities in coverage of iron and vitamin A supplements, and anthelminthic medication among children in the Dominican Republic.

E N D
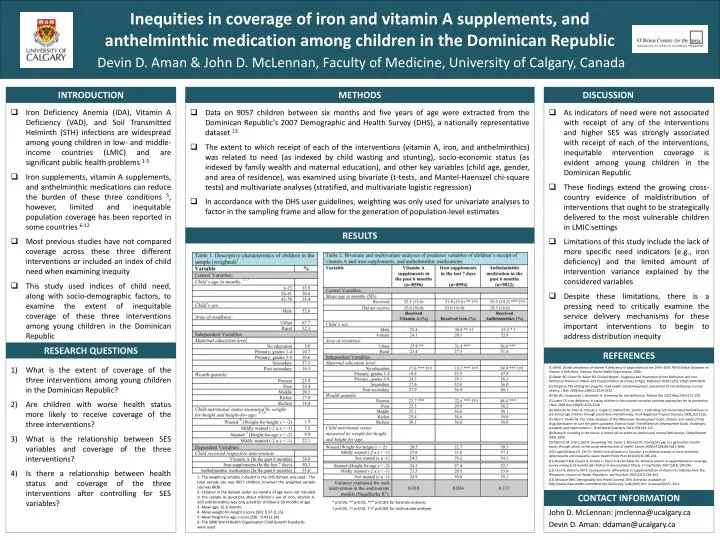
Inequities in coverage of iron and vitamin A supplements, and anthelminthic medication among children in the Dominican Republic Iron Deficiency Anemia (IDA), Vitamin A Deficiency (VAD), and Soil Transmitted Helminth (STH) infections are widespread among young children in low- and middle-income countries (LMIC) and are significant public health problems 1-5 Iron supplements, vitamin A supplements, and anthelminthic medications can reduce the burden of these three conditions 5, however, limited and inequitable population coverage has been reported in some countries 6-12 Most previous studies have not compared coverage across these three different interventions or included an index of child need when examining inequity This study used indices of child need, along with socio-demographic factors, to examine the extent of inequitable coverage of these three interventions among young children in the Dominican Republic INTRODUCTION RESEARCH QUESTIONS Data on 9057 children between six months and five years of age were extracted from the Dominican Republic's 2007 Demographic and Health Survey (DHS), a nationally representative dataset 13 The extent to which receipt of each of the interventions (vitamin A, iron, and anthelminthics) was related to need (as indexed by child wasting and stunting), socio-economic status (as indexed by family wealth and maternal education), and other key variables (child age, gender, and area of residence), was examined using bivariate (t-tests, and Mantel-Haenszel chi-square tests) and multivariate analyses (stratified, and multivariate logistic regression) In accordance with the DHS user guidelines, weighting was only used for univariate analyses to factor in the sampling frame and allow for the generation of population-level estimates METHODS RESULTS DISCUSSION As indicators of need were not associated with receipt of any of the interventions and higher SES was strongly associated with receipt of each of the interventions, inequitable intervention coverage is evident among young children in the Dominican Republic These findings extend the growing cross-country evidence ofmaldistributionof interventions that ought to be strategically delivered to the most vulnerable children in LMIC settings Limitations of this study include the lack of more specific need indicators (e.g., iron deficiency) and the limited amount of intervention variance explained by the considered variables Despite these limitations, there is a pressing need to critically examine the service delivery mechanisms for these important interventions to begin to address distribution inequity REFERENCES (1) WHO. Global prevalence of vitamin A deficiency in populations at risk 1995–2005. WHO Global Database on Vitamin A Deficiency. Geneva, World Health Organization, 2009. (2) Baker RD, Greer FR, Baker RD. Clinical Report - Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0-3 Years of Age). Pediatrics 2010 11/01;126(5):1040-1050. (3) Chaparro CM. Setting the stage for child health and development: prevention of iron deficiency in early infancy. J Nutr 2008 Dec;138(12):2529-2533. (4) Wu AC, Lesperance L, Bernstein H. Screening for iron deficiency. Pediatr Rev 2002 May;23(5):171-178. (5) Lutter CK. Iron deficiency in young children in low-income countries and new approaches for its prevention. J Nutr 2008 Dec;138(12):2523-2528. (6) Albonico M, Allen H, Chitsulo L, Engels D, Gabrielli AF, Savioli L. Controlling soil-transmitted helminthiasis in pre-school-age children through preventive chemotherapy. PLoS Neglected Tropical Diseases 2008;2(3):e126. (7) Allen T, Parker M. The 'other diseases' of the Millennium Development Goals: rhetoric and reality of free drug distribution to cure the poor's parasites. (Special Issue: The Millennium Development Goals: challenges, prospects and opportunities.). Third World Quarterly 2011;32(1):91-117. (8) Strang B. Investing in the future: A united call to action on vitamin and mineral deficiencies, Global Report 2009. 2009. (9) Marmot M, Friel S, Bell R, Houweling TAJ, Taylor S, Marmot M. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet 2008;372(9650):1661-1669. (10) LopezCevallos DF, Chi CH. Health care utilization in Ecuador: a multilevel analysis of socio-economic determinants and inequality issues. Health Policy Plan 2010;25(3):209-218. (11) Bendech MA, Cusack G, Konate F, Toure A, Ba M, Baker SK. National vitamin A supplementation coverage survey among 6-59 months old children in Guinea (West Africa). J TropPediatr 2007;53(3):190-196. (12) Choi YJ, Bishai D, Hill K. Socioeconomic differentials in supplementation of vitamin A: evidence from the Philippines. Journal of Health, Population and Nutrition 2005;23(2):156-164. (13) Measure DHS: Demographic and Health Surveys. DHS Overview. Available at: http://www.measuredhs.com/What-We-Do/Survey-Types/DHS.cfm. Accessed 09/27, 2011. CONTACT INFORMATION John D. McLennan: jmclenna@ucalgary.ca Devin D. Aman: ddaman@ucalgary.ca What is the extent of coverage of the three interventions among young children in the Dominican Republic? Are children with worse health status more likely to receive coverage of the three interventions? What is the relationship between SES variables and coverage of the three interventions? Is there a relationship between health status and coverage of the three interventions after controlling for SES variables? Devin D. Aman & John D. McLennan, Faculty of Medicine, University of Calgary, Canada 1- The weighting variable included in the DHS dataset was used. The total sample size was 9057 children, however the weighted sample size was 8638 2- Children in the dataset under six months of age were not included in the sample as questions about children’s use of iron, vitamin A, and anthelminthics was only asked for children 6-59 months of age 3- Mean age: 32.8 months 4- Mean weight-for-height z-score (SD): 0.37 (1.15) 5- Mean height-for-age z-score (SD): -0.43 (1.34) 6- The 2006 World Health Organization Child Growth Standards were used * p<0.05, ** p<0.01, *** p<0.001 for bivariate analyses † p<0.05, †† p<0.01, ††† p<0.001 for multivariate analyses






