Download
1 / 17
170 likes | 193 Views
Sources of Dissatisfaction in Albanian Health Care System. Zamira Sinoimeri, MD, MSC Deputy Minister of Health Albania. Purpose. To present: Sources of Dissatisfaction in the Albanian Health System The need to reconfigure the health care system

E N D
Sources of Dissatisfaction in Albanian Health Care System Zamira Sinoimeri, MD, MSC Deputy Minister of Health Albania
Purpose To present: • Sources of Dissatisfaction in the Albanian Health System • The need to reconfigure the health care system • The strategies needed to face the problems and overcome the challenges,
Definition • Sources of Dissatisfaction (SoD) are all those faults in the health system that lead into low utilization of health care services (both curative and preventive); and eventually a deteriorating and vulnerable health status of the population.
System approach: Organization Financing Quality of service Utilization Focus/Resource distribution Disconnect People approach: Bypassing Informal payments Low HI enrollment Low awareness about HI Detailed Review of SoD
SoD: System - Organization • Unclear roles and responsibilities of major players: MoH, HII, Public Health/PHC directories in the districts. • Re-organization of district structures into regional ones.
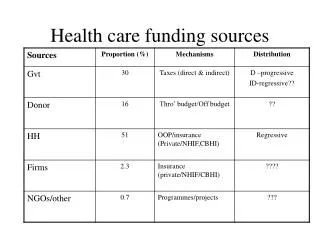
SoD: System - Financing • Low public funding for health. • Health insurance scheme covers only PHC. • Low health insurance enrollment. • The public health financing is fragmented and fails to give providers the incentives for efficiency and quality improvements, nor it establish clear lines of accountability. • Provider payment that does not follow performance. • Wide-spread informal payments.
SoD: System – Quality of Service • Perceived quality of service is low (bypassing in PHC, export of patients in hospital sector) • Few of health personnel have received formal training after their graduation. • More investments are needed to modernize the system
SoD: System – Utilization • Low utilization of services in both the primary and secondary health care (hospital bed occupancy rate: 50%) . • The amount of PHC services provided in the hospitals are not recorded, this fuels the IP mechanism • Ability to diagnose and treat needs improvement.
SoD: System – Resources • Services are oriented into the curative services and less into preventive ones. • 90% of PHC physicians have no training as Family Doctors • System should have better priorities (epidemiologic shift into chronic illnesses) • Only a part of health personnel have received formal training after their graduation
SoD: System – PHC- Hospital Sector disconnected • Primary care is isolated from secondary care. • Health insurance covers only PHC. • PHC patients bypass their facilities of coverage to be treated in polyclinics and hospitals (at higher costs). • Weaker PHC means more informal payments to secondary level and inefficient PHC.
SoD: People - Bypassing • 50% of people, especially in rural areas bypass their PHC facility of coverage to go to polyclinics and hospitals in urban districts. • They incur more costs (transportation, examinations, work-day lost, informal payments to personnel) • Increased burden of disease.
SoD: People – Informal Payment. • Over 93% of people seeking care pay for smth, most of it as informal payments. • IP often cause frustration to patients and delays in seeking care. • Half of health expenditures are of informal nature, often hampering access of patients to health services. • IP, mostly at secondary level, cause increased burden of disease.
SoD: People – Health Insurance • Population is not fully aware of the benefits of HI scheme and the procedures of getting enrollment. • HI covers PHC and not secondary level. • Penalties in form of user fees for uninsured are often channeled as IP to medical personnel.
Some reforms introduced • Changes in financing; • Reduction of the excess capacity of the provision network • Some decentralization; • The introduction of some private initiative • Setting up CME & National Center for Quality and Accreditation • Limited impact - Public perception is still low;
Strategies needed to face the problems and overcome the challenges (1) • The main challenge is the shift from hospitals to PHC • Health System in Albania needs a reform of its organization, financing to increase efficiency, improve quality of service and have the people in its focus. • The aim of financial reform is to put all public sector funding for health in a single pool. • Re-orient services in line with actual priorities; • Provider payments should award performance. • Health sector reform calls for a cross-sectorial approach.
Strategies needed to face the problems and overcome the challenges (2) • Health care reform requires government workforce planning, and more active policies influencing the education and training • The reform process calls for a strong involvement of all in-country and outside assistance, in a clear timeline and identified milestones. • Full transparency to stakeholders and the public is necessary.