Download
1 / 27
270 likes | 387 Views
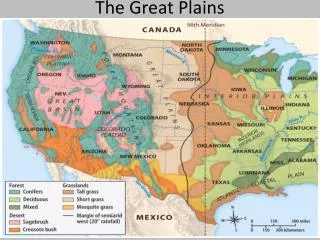
Health Care Policy for the Great Plains Bismarck, North Dakota. October 16, 2001 Mary Wakefield Ph.D., RN, FAAN George Mason University. Catalysts for Health Policy. FINANCING. ACCESS To Care. Rural Health Care. QUALITY. Rural Challenges: Population Characteristics.

E N D
Health Care Policy for the Great PlainsBismarck, North Dakota October 16, 2001 Mary Wakefield Ph.D., RN, FAAN George Mason University
Catalysts for Health Policy FINANCING ACCESS To Care Rural Health Care QUALITY
RuralChallenges: Population Characteristics • Proportion of elderly • Chronic conditions • Underutilization of health services • More uninsured • Lower average income • Higher incidence of specific health problems
Source: U.S. Department of Commerce, Bureau of the Census, Current Population Survey. March 1997
RuralChallenges: Population Characteristics • Proportion of elderly • Chronic conditions • Underutilization of health services • More uninsured • Lower average income • Higher incidence of specific health problems
Rural Health Risk Factors: • Adolescents most likely to smoke • Adults most likely to smoke • Alcohol consumption higher among adults living in non-metro counties • Obesity higher for women and men • Physical inactivity CDC - Health, United States, 2001
Rural Mortality • Children and young adult death rates in the most rural counties were over 50 percent higher than rates in fringe counties • Death rates among seniors • Ischemic heart disease over 20 percent higher in most rural counties • Chronic obstructive pulmonary disease among men 30 percent higher in non-metro counties • Suicide rates increase steadily as counties become less urban • Infant mortality rates (South and West) non-metro counties had the highest rates. CDC - Health, United States, 2001
Other Urban-Rural Health Measures • Limitation in activity due to chronic health conditions among adults, more common in non-metro counties • Total tooth loss among seniors increases as urbanization declines CDC – Health, United States, 2001
Ten Essential Public Health Services • Monitor health status to identify community health problems. • Diagnose and investigate health problems and health hazards in the community. • Inform educate, and empower people about health issues. • Mobilize community partnerships to identify and solve health problems. • Develop policies and plans that support individual and community health efforts Stabilizing the Rural Public Health Infrastructure, National Advisory Committee on Rural Health, June 1999
Rural Challenges:Delivery System Characteristics • Low population density with increased travel times to health care • Healthcare facilities with low volume fixed overhead • Financial fragility • Health care provider shortages
Impacts on Workforce:Health Care • Aging U.S. population • Increasing ethnic/cultural diversity of U.S. population • Technology
Characteristics of RN Workforce • Aging RN workforce • Enrollment • Shortage of specialty nurses • Geographic maldistribution ofnurses
Physician Workforce Trends • GME funding • Policies are oriented to acute care training • Growth of non-physician clinicians • Growing ratio of women in medicine • Emerging role of the Hospitalists • Only 12% of current medical school enrollees are minorities
Report Vacancy Rates (Percent) AHA 2001
Workforce Questions • What strategies will improve the recruitment and retention of healthcare professionals? • What strategies will improve the recruitment, retention and leadership capacity of health system managers and policy makers? • How can the particular health human resource needs of rural regions be met in a sustainable and cost-effective fashion?
Landmark State Legislation • California mandates RN:Patient ratios • CA Department of Health to develop ratios for minimum requirements. • Bans unsafe “floating” of nurses to units without orientation
Federal Level Workforce Programs • AHECs • NHSC • Burdick Interdisciplinary Training Program • Title VII, VIII • Medicare: GME/IME • New Legislation
Policy Considerations to Improve Access to Rural Health • Evaluate varying definitions of rural • Data • Priority to academic programs with rural emphasis • Support training in outpatient settings • Capitalize on the strengths of every discipline • Bonus payments • Strengthen Federal programs that work
Additional Policy Considerations • Prescription Drug Benefit • Bio-terrorism / Public Health
Rural Health Care Delivery Systems and the Economic Health of Communities • Health care service is a vital sector of the local economy – as important as, utilities, schools, and local industry. • A deliberate community investment to retain local health expenditures.
Cooperative Approach • Solutions vary, but the process has common elements: • realization that cooperation with regional neighbors can produce more. • realization that communities have health profiles and that investing in prevention is cheaper than paying for cures.
“We all share the same sky . . . . . . . we just have different horizons.”