Download
1 / 33
330 likes | 511 Views
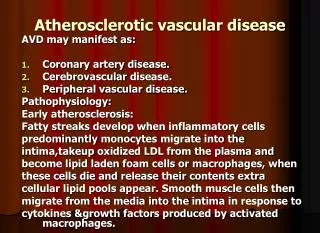
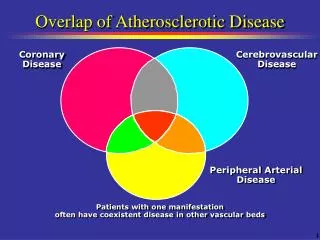
Atherosclerotic coronary vascular disease. leading cause of death in the U.S. !! men > 40 y.o. women > 50 y.o. declining rates since 1980 : 42 % !! lifestyle alterations 7-9 million Americans. Atherosclerotic coronary vascular disease. ASYMPTOMATIC ~ 50 % SYMPTOMATIC ~ 50 %

E N D
Atherosclerotic coronary vascular disease • leading cause of death in the U.S. !! • men > 40 y.o. • women > 50 y.o. • declining rates since 1980 : 42 % !! • lifestyle alterations • 7-9 million Americans
Atherosclerotic coronary vascular disease • ASYMPTOMATIC ~ 50 % • SYMPTOMATIC ~ 50 % • ISCHEMIC HEART DISEASE = ANGINA
Platelet clumping Fibrin PLAQUE RUPTURE AND BLOOD CLOTTING IN AN ATHERO-SCLEROTIC BLOOD VESSEL Red blood cells Red blood cells and fibrin Platelet plug
HMG COA REDUCTASE INHIBITORS Use of HMg COAs can reduce cholesterol by 35%. * Should not be used with cyclosporine, niacin, gemfibrozil - myositis; however no reports with fluvastatin
Atherosclerotic coronary vascular disease • RISK FACTORS • age and sex • genetics; family history • serum lipid levels • HTN • tobacco ( smoking) • elevated blood glucose
ISCHEMIC HEART DISEASE • ASCVD: coronary arteries>>> decreased blood supply to myocardium= ischemia >>>pain= ANGINA • May be slowly OR rapidly progressive; with or without symptoms
ISCHEMIC HEART DISEASE • ANGINA : most common cause= ASCVD • also HTN • anemia • RHD • CHF
CARDIAC ARREST • sudden cardiac death • >90% associated with underlying CVD • 30 % of all natural deaths in U.S. • cardiac arrhythmias: ventricular fibrillation • most common in early am
ANGINA PECTORISstatus • initial; exertional or at rest; LEVEL • STABLE vs. PROGRESSIVE • FREQUENCY- SEVERITY- CONTROL • brief chest pain ( 1-3 minutes) • ususally size of fist in mid-chest • aching, squeezing, tightness • may radiate, left shoulder, arm, mandible, palate, tongue
ANGINA PECTORIS • DENTAL OFFICE • STRESS, ANXIETY, FEAR>>>> release of endogenous epinephrine>>> increased HR, BP ( HR x MAP > 12,000 !!) >>> increased cardiac load, O2 demand>>> additional epinephrine ( LA) >>> exacerbated angina
ANGINA PECTORIS • MEDICAL MANAGEMENT • exercise, weight loss, diet, smoking cessation, other medical conditions control: diabetes, HTN, thyroid, anemia, arrhythmias • DRUGS: vasodilators ( NGN), etc.
ANGINA PECTORIS • DRUGS • vascular dilators: alleviate coronary artery spasms; open up occluded vessels, increase blood flow • NGN, under tongue, transdermal patches • longer acting NITRATES
ISCHEMIC HEART DISEASE • LABORATORY TESTS • chest radiograph, fluoroscopy • EKG • echocardiography • technicium Tc 99 scan • enzymes ( LDH, ALT, AST) • angiography
DENTAL MANAGEMENT for ANGINA PECTORIS • mild diagnosed, monitored infrequent symptoms use NGN <2 x week; exertion only easily controlled • moderate diagnosed, ± monitored occasional symptoms use NGN <5 x week; exertion easily controlled
DENTAL MANAGEMENT for ANGINA PECTORIS • severe diagnosed, ± monitored ± frequent symptoms use NGN <8 x week; exertion not necessarily well controlled
DENTAL MANAGEMENT for ANGINA PECTORIS • mild most dental tx vitals, sedation • moderate simple tx vitals, sedation ± prophylactic NGN vitals, sedation + routine tx prophylactic NGN oxygen complex tx HOSPITALIZATION
DENTAL MANAGEMENT for ANGINA PECTORIS • severe simple tx vitals, sedation + prophylactic NGN • routine-complex tx HOSPITALIZATION
Surgical Treatment • Coronary Artery By-Pass Graft (CABG) • Saphenous vein • Internal mammary artery • Radial artey
Dental Considerations - CABG • The CABG is not considered a risk condition for BE, therefore antibiotic prophylaxis is not necessary • Avoid use of vasoconstrictor for the first 3 months due to electrical instability of the heart during this period
Post-Myocardial Infarction “MI”, “Coronary”, “Heart Attack” Infarction - an area of necrosis in tissue due to ischemia resulting from obstruction of blood flow
Prognosis After Infarction • Hospital discharge after 7 days • 50% of survivors are at increased risk of further cardiac events • Without further treatment, 5-15% will die in first year; similar number will have reinfarction • With treatment, morbidity and mortality markedly reduced (<3% in GUSTO trial)
MYOCARDIAL INFARCTION • CAUSES of DEATH from MI • ventricular fibrillation • cardiac arrest • congestive heart failure • cardiac tamponade • thromboembolic complications
MYOCARDIAL INFARCTION • history of past -MI • best to wait >6 months= NO ROUTINE CARE! If so, AHA prophylaxis • physical status, Rxs, vital signs, fatigue, CHF, cardiac reserve • CLOSE MONITORING !! • MEDICAL CONSULTATION
MYOCARDIAL INFARCTION • short, non-stressful appointments schedule at BEST time for patient • changes>>>> STOP- POSTPONE dental tx sedation : N2O2 • good anesthesia, pain control, anxiety reduction, etc. • prophylactic oxygen ( nasal cannula) ± NGN; ALWAYS have NGN available!
MYOCARDIAL INFARCTION • NO EPINEPHRINE • anticoagulants( Coumadin) • PT or INR, BT • arrhythmias • CHF • Rxs: side-effects, interactions, adjustment