Download
1 / 35
350 likes | 486 Views
Social Capital and Wellness Amongst First Nations in Coastal British Columbia. Ralph Matthews, Ph.D., Professor of Sociology, The University of British Columbia, And Professor Emeritus of Sociology, McMaster University Chris Buse, BA The University of British Columbia

E N D
Social Capital and Wellness Amongst First Nations in Coastal British Columbia Ralph Matthews, Ph.D., Professor of Sociology, The University of British Columbia, And Professor Emeritus of Sociology, McMaster University Chris Buse, BA The University of British Columbia Presentation to a Symposium on “Aboriginal Experiences of Aging” Saskatoon, Saskatchewan, September 17-19, 2008
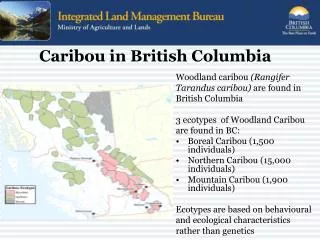
Present Data on Health from Two Studies • Coastal Communities Project (CCP) • Working with Six First Nation Communities and Six Adjacent Civic Communities in Coastal B.C. • Issues of Environment, Resource Management, Education, Governance, and Health. • Funded through the SSHRC ‘Community-University Research Alliance (CURA)’ Program. • Resilient Communities Project (RCP) • Social Capital and Economic Development 23 Coastal Communities in British Columbia. • Funded through the SSHRC ‘Initiatives on the New Economy’ Program.
1.I : Coastal Communities Project : Investigating Health in Old Massett • Old Massett Band Council (Haida Gwaii) wished to have a community interview study carried out on a range of issues. • Appointed Councilors who worked with us on designing it. • All interviews conducted by members of the Band. • Health and health care was one of the topics covered. • Focus was on: • Who consulted for health care assistance. • Asked about use of traditional healing versus western medicine.
The Social and Cultural Basis of Wellness and Healing • When asked who they had consulted in the past 12 months about a physical or mental health issue and how frequently, many of the ‘consultations’ identified medical advice was obtained from family, friends and non-medical personnel (see Table 1). • When asked about using traditional healing methods, 40 percent of males and 34 percent of females had done so. • (32 percent of females and 7 percent of males did not indicate receiving advice regarding any health problems)
Table 1: Old Massett – Persons Contacted and Frequency of Contact Regarding Health
Traditional Healing • Most respondents received traditional healing from family and friends. • Traditional healing methods were applied to a range of health issues from arthritis, to common colds, to cancer. • Respondents were least likely to seek traditional healing for broken bones and for eye and tooth problems. • All but one respondent who sought traditional healing declared it to have been successful. • Interviewers were sometimes provided with detailed descriptions for the preparation of traditional medicines – knowledge that we regard as the cultural knowledge of the Haida people. • Throughout coastal B.C. we have been consistently informed about traditional healers from the northwest of the USA (notably Montana, Utah) who complete a circuit of First Nation communities in the Pacific Northwest utilizing/selling a variety of traditional medicines.
Indigenous Healing and Wellness in Social Context • The point of beginning our discussion with our Old Massett data is to demonstrate that: • Health care and healing always occurs in a social context. • This is particularly the case when dealing with indigenous persons’ health care where an awareness of the social and cultural context is critically necessary in order to understand virtually all aspects of health care. • The social and cultural context retains strong elements of traditional knowledge and healing, operating where more ‘western’ healing and healthcare processes take place. • Let us turn now to a more quantitative investigation of that social context – using the findings of the Resilient Communities Project (RCP) to examine the relationships involved.
II. The Resilient Communities Project (RCP): Examining ‘Health’ in Social Context • Five year Study –Multi-stage project involving: • Background Data. • Statistical data analysis of pre-existing data. • Mailed Questionnaire. • Sent to 4,386 households in 23 communities. • N.B.: Five mailings – 60.0 % response rate. • Interviews (Semi-Structured). • 93 local residents from six communities. • 78 ‘leaders’ from six communities. • All households on two First Nation reserves.
Measuring Social Capital in the RCP: • Social Capital seen as an attribute of the access that people have to ‘resources’ through their contact with other persons within their social network. • Refers to embedded social relations entrenched in social ties (Granovetter 1985). • We define social capital as resulting in the ‘social ties’ that people have with one another. • Embodied through strength of ties between individuals or groups that foster norms of trust, reciprocity, social participation and civic engagement (Putnum 2000; Burt 2001; Coleman 1990) • The RCP measures social capital in terms of the extent to which people have strong ties (i.e. friends and relatives) and weak ties (acquaintances) with people who reside inside or outside their communities, and who have potential access to important social and economic resources (measured with a Position Generator).
Role of Trust in Relation to Social Capital • Trust can be seen as both a precondition for the cooperation that allows social capital relations to form. • Trust is also the result or outcome of these social relations. • In the context of healthcare and wellness trust provides or produces: • access to resources • allows for greater efficiency in healthcare services delivery and traditional healing • Networks of social support • Higher trust = higher levels of wellness (Rose 2000).
Measuring Trust in the RCP: • Respondents were asked to indicate support or disagreement with 12 statements concerning trust. • Statements ranged from ‘global’ measures (e.g. Most people can be trusted), to ‘community specific’ measures (e.g. Business leaders in this community can be trusted). • Factor Analysis of our ‘Trust’ variables identified two distinct factors comprising seven of the 12 statements. • We have labeled these Generalized Trust and Institutional Trust.
Measuring Health and Wellness in the RCP: • General Well-Being / Wellness: • “All things considered, how satisfied are you with your life as a whole these days?” • (Dissatisfied to Satisfied on a 10 point scale) • Physical Well-Being: • “How would you describe the state of your health compared to other persons your age?” • Poor; Fair; Good; Very Good; Excellent • Psychological Well-Being: • “How much of the time, over the past two weeks, have you: Been a nervous person; Felt calm and happy; Felt down-hearted and blue; Been a happy person; Felt so down in the dumps that nothing could cheer you up?’ • All; Most; Some; Little; or None of the time. • Calculated a 16 point scale constructed from the questions above
Other Variables in Our Analysis: • Age • In years as of 2004 • Income • Measured in five categories • Education • Measured in four categories • Ethnic Status • First Nation versus Non-First Nation
Traditional Indicators of Health Health and Wellness
Summary of Findings Comparison: First Nation and Non-First Nations Respondents: • F.N. persons have significantly lower household incomes, significantly lower educational levels. • F.N. persons have significantly higher formal and informal social participation (i.e. the basis of social capital) • Formal (17 point index) = scheduled formal meetings for sports teams, arts and crafts, FN ceremonies, etc. • Informal (15 point index) = going out for drinks, movies, etc. • F.N. have significantly lower levels of trust: • Note contradiction with most social capital literature that sees trust as being directly associated with social participation. • F. N. persons have significantly lower of levels of all three measures of wellness and health • i.e. General wellness; Physical Health; Mental Wellness.
Means Comparison – F. N. versus Non-F. N. : All Social Capital and Trust Variableswith All Wellness and Health Variables
Review of our Findings regarding the Context of Trust • Many studies of the social determinants of health emphasize the role of social capital (i.e. networks and involvement in social relations) in ‘health’. • We have used measures of involvement in formal and informal groups as our proxy measure of this. • We see significant differences between F.N. and non-F.N. persons in terms of their involvement in formal and informal groups (i.e. F.N. persons are more likely to be involved in both formal and informal groups). • Many studies of social capital demonstrate that the more people are involved in community formal and informal activities within their community, the more likely they are to trust community members. • We see that there are significant differences between First Nation and Non-First Nation persons in terms of trust. • First Nation persons are likely to have less trust than non-First Nation persons. • The more First Nation persons are involved in formal and informal groups/activities in their community the LESS likely they are to trust members of their community. • Now let us look at the relationship between trust, wellness and other social variables.
Building a Model of Wellness and Its Relationship to Trust • Statistical models set up to explain the relationship between Trust and Wellness • Bi-variate statistics illustrate trust disparities and relationship directionality. • In other studies, trust is rarely modelled as the primary explanatory variable of health; it is generally something to be controlled. • Hypothesis not formally tested amongst F.N. populations in Canada. • Three measures – general wellness; physical health; mental health • Wellness is argued as a more stable measure of health and well-being; going beyond physical health and attempting to encompass a greater social depiction of an individual’s life. Therefore, it is most important in our considerations. • Literature suggests that trust may have implications for health. (Veenstra 2000; Hardin 2002; Rose 2000; Kawachi 1999).
F.N. Findings: It’s all about Generalized Trust • Generalized Trust is a significant predictor of all three health measures (Higher Trust = Better Health). • Institutional trust suppresses original trust relationship; controlling for it makes Generalized Trust/Health association stronger (Has no effect on health and wellness on its own). • Social participation has little to no effect on the trust/health association, and little to no influence on wellness more generally. • This seems contradictory to evidence presented in the social capital literature. • We would expect higher social participation to produce better health. • Variance – the proportion of health and wellness explained by trust is high
F.N. Findings: Traditional Predictors of Health • Age is not a significant predictor of health and wellness • Education • Importance of H.S. Diploma, but results are not statistically significant • Achieving more than a H.S. Diploma does not seem to produce greater levels of wellness as indicated in the literature • Income • Income is not as important to this relationship as trust is, and for the most part, income is not significantly associated with health; contradicts traditional literature on health • a threshold effect is present; that is, individuals occupying the lowest income category are worse off, but occupying successively higher income categories is not necessarily better for health or wellness • Variance • Age and Education do not explain health and wellness outcomes • Income accounts for a little less than half of health and wellness (still not as much as generalized trust)
Limitations • Small sample size • Social Participation – What gives? • RCP data may not be asking the right questions: • Does not adequately address social activity around family ties or family relations • To look at health, wellness, and healing, we need to analyze social relationships, not just social participation • Data need to reflect the way in which First Nation respondents engage in activities; family may play a more important role than First Nation community activities
Policy Directions: Towards a CHED Model • CHED Model – Community Health and Economic Development • Developed by Glen Timbers, Director of United Church Health Services, Bella Coola, BC. • A service delivery model that focuses on the community basis of health and the development of trust – particularly with F. N. communities. • Building Community requires meaningful participation from members • Sees ‘health’ and ‘wellness’ as a community based phenomenon related to the economic and social well-being of a community. • The CHED Model is centred around the development of community based generalized trust. Our findings show that this is a dominant factor in self-reported physical and mental health and general well-being, particularly for First Nation communities.
Central Coast Health and Well-Being Charter • Central Coast Health and Well-being Charter • Agreement to work on local strategies to improve service delivery, to strengthen community bonds and to promote relationships, spirit and service networks of communities. • CHED depends on: leadership, learning and development systems; social and recreational activities; unique history, location and social attributes; work and economic activity; infrastructure and environment; health services; governance and coping systems • Signed by Five First Nation Band Communities and all non-First Nation Communities.
Policy Directions: Towards a CHED Model • Healing and wellness are social processes requiring social considerations • Wellness is a resource for daily life • Health services need incorporate and respect traditional medicines/values as an integral part of the economic, social, and spiritual community • Addressing trust may be more beneficial to health than palliative care • Community Involvement • Needed to influence regional authorities, independent community service providers, and provincial/federal governments • Band Unity via Trust Building; Community Gardens • Cross-cultural issues are important when dealing with healing and wellness
References Burt, R.S. (2001). Structural Holes Versus Network Closure as Social Capital. Social Capital: Theory and Research, Eds. Nan Lin, Karen Cook, & Ronald Burt. New York: Aldine De Gruyter. Pp. 31-56. Central Coast Regional District. (2005). Central Coast Health and Well-being Charter. Charter Implemented on July 24, 2006 by Wuikinuxv Nation, Nuxalk Nation, Heiltsuk Nation, Kitasoo Nation, Bellac Coola General hospital Board, RW Large Memorial Hospital Board, Central Coast Regional District, and United Church Health Services. Coleman, J. (1990). Relations of Trust. Foundations of Social Theory. Cambridge, MA: The Belknap Press of Harvard University Press. Pp. 91-116. Granovetter, M.S. (1985). Economic Action and Social Structure: The Problem of Embededness. The American Journal of Sociology, 91(3): 481-510. Hardin, R. (2002). Trust and Trustworthiness. New York: Russel Sage Foundation. Kawachi, I., et al. (1999). Social Capital and Self-Rated Health: A Contextual Analysis. American Journal of Public Health, 89(8): 1187-1193. Putnum, R. (2000). Bowling Alone: The Collapse and Revival of American Community. New York: Simon and Schuster. Rose, R. (2000). How Much Does Social Capital Add to Individual Health? A Survey Study of Russians. Social Science and Medicine, 51(9): 1421. Timbers, G. & FitzZaland, R. (2003). Community Health and Economic Development Model: For Healthy Communities. Presentation made to VCH Accreditation Team. Veenstra, G. (2000). Social Capital, SES and Health: An Individual-Level Analysis. Social Science and Medicine, 50: 619-629. Veenstra, G. (2007). Social Capital and Health in Canada: Compositional Effects of Trust, Participation in Networks, and Civic Activity on Self-Rated Health. Social Capital, Diversity, and the Welfare State, Eds. F.M. Kay and R. Johnson. Vancouver, BC: UBC Press.
THANK YOU! • For more information: • Websites: • Resilient Communities Project • www.resilientcommunitiesproject.ca • Coastal Communities Project • www.coastalcommunitiesproject.ca • E-MAIL: ralph.matthews@ubc.ca