香港政府華員會 暨 護士分會、登記護士分會、香港護士總工會主辦 廣州、香港防護 SARS 經驗交流會 日期: 2003 年 5 月 3 日 題目: 互相關懷,互相支持,互相監察
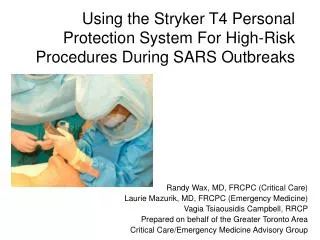
香港政府華員會 暨 護士分會、登記護士分會、香港護士總工會主辦 廣州、香港防護 SARS 經驗交流會 日期: 2003 年 5 月 3 日 題目: 互相關懷,互相支持,互相監察 防止醫護人員及病人受感染 講者: 新界東醫院聯網風險管理及質素保證總監 雷兆輝醫生. w.e.f. Tuesday 8 April 2003 Main task To prevent secondary infection of SARS amongst health care workers and patients

香港政府華員會 暨 護士分會、登記護士分會、香港護士總工會主辦 廣州、香港防護 SARS 經驗交流會 日期: 2003 年 5 月 3 日 題目: 互相關懷,互相支持,互相監察
E N D
Presentation Transcript
香港政府華員會 暨 護士分會、登記護士分會、香港護士總工會主辦香港政府華員會 暨 護士分會、登記護士分會、香港護士總工會主辦 廣州、香港防護SARS經驗交流會 日期:2003年5月3日 題目: 互相關懷,互相支持,互相監察 防止醫護人員及病人受感染 講者: 新界東醫院聯網風險管理及質素保證總監 雷兆輝醫生
w.e.f. Tuesday 8 April 2003 Main task To prevent secondary infection of SARS amongst health care workers and patients Mutual care, support and monitoring互相關懷,互相支持,互相監察 Protect yourself, your colleagues and your family Strictly follow all recommended infection control measures all the time. Don’t give yourself a life threatening present (SARS). Dr. SF Lui, SD (RM&QA), NTEC NTE0309a 030412
311HKSAR- SARS E ? East wind,East Side E-Block of Amoi Garden, AHNH, Ease of Spread
Mr. C’s family tree (n = at least 189, 49 case unclassified yet) Layer 1Layer 2 (n=128) (n=61) > Index case’ relatives 5 2 friends HEALTH CARE WORKERS73 13 FM > 8 A&E staff (during 2 visits by index case) > 6 Doctors attended index case (out of 7) > 5 Doctors visiting ward 8A > 9 Examiners of Med 3 students (out of 11) > 8 Med 3 students taking clinical exam (out of 20) > 9 Med 5 students visited ward 8A > 15 Ward 8A nursing staff (out of 17) > 6 Ward 8A HCA / WA > 3 Physiotherapists visited ward 8A > 2 EMSD visited ward 8A > 2 Other staff visited ward 8A PATIENTS / VISITORS of ward 8A 50 4 FM, 2 GP > 25 patients (15 discharged, 10 not discharged) > 25 visitors > 40 HCW
Case study (1) M30, SLE, on haemodialysis at PWH. Work in ShenZhen 15/3/03 claimed OK on arrival at HD centre Looked unwell, temp 38C. Admitted to having fever for 1 days CXR: RLZ changes. WCC 6.0, lymphocytes 0.7 Dx: Atypical pneumonia. Admitted to AP ward NPA: Influenza A Clinical improvement. Discharged on 19/3 Stay with brother on 19/3 before going back to ShenZhen Return to PWH on 22/3, fever, SOB, respiratory distress CXR: diffuse changes. Admitted ITU Dx: SARS 2 Diagnosis: ? Influenza A + SARS [note: lymphocyte count remained low] Secondary spread > brother (fever on 23/3) > ? 321 cases at Amoi Garden > 2 renal nurses at renal unit
Case study (2) F80, COAD, admitted from OAH with #NOF Day 1 post-op: afebrile, SOB, desaturation Day 2: CXR bilateral pulmonary infiltrate Dx: Aspiration pneumonia Isolated in side room Day 8: Died, ARDS, DIC, ARF PM: Atypical pneumonia Likely admitted with AP/SARS ? Atypical presentation: afebrile in elderly [Note: day 3, WCC 14.1, Lymphocyte count 0.4 (3%)] >> no outbreak (? in side room)
Case study (3) E1 of AHNH 2 cases of chest infection admitted into Medical ward Subsequent suspected SARS, transferred to PMH 1 patient in side room, 1 patient in open cubicle Protection for nurse - standard + mask Nursing suspected AP patients without adequate precaution and infection control measures Secondary spread > 1 ward nurse (fever 25/3) > 3 ward nurse + 1 SS (fever 31/3) > 1 HCA + 1 doctor + 1SS (fever 7/4) HCW = 8 > 2 ward patient + 3 suspected > 4 ex-ward patients at TPH > 1 ex-wardpatient at SH > 1 discharged + 1 suspected Patient = 8 +4S
Case study (4) E3 and E6 of AHNH M80, admitted to surgical ward E3 with PR bleeding Day 4: fever, chest infection Dx: Strep. Pneumonia, UTI (E coli and Kleb) Transferred to Medical ward (E6), Day 6: Died Likely typical pneumonia + AP/SARS [lymphocyte count 0.4 only] Secondary spread On ward E3> 1 HO, 1 Nurse, 1 HCA (fever 29/3, 30/3)> 1 A&E MO who saw HCA(fever 4/4) HCW = 4> 2 patient and 9 ex-patients Patient = 11On ward E6 > 1 MO, 10 Nurses, 1 HCA, 1 WC HCW = 13> 8 in-patients + 5 suspected> 9 ex-patients + 2 suspected Patient = 14> 3 Visitors Visitor = 3> secondary spread at OAH Layer 2 = 4
OUTBREAK OF SECONDARY INFECTION OF SARS AMONGST HEALTH CARE WORKERS AT PWH– REVIEW AND RECOMMENDATION • Structural problem • 1. PWH is not an infection disease hospital. The isolation and supporting facility are not appropriate nor adequate. • Unexpected / rapid accumulation of a large number of patients • 2. Unexpectedness of the outbreak. No preparation for the outbreak. • The tremendous caseload (70 HCW over a few days only) • Necessary to draft in temporary nursing staff from other ward / dept • 5. Viral load on the ward was likely to be very high.
Staff issues • 6. Most of the staff did not attended structured briefing on • management of SARS case before commencement of duty (too busy) • 7. Problem with using the N95 mask – correct size, too stuffy, not tolerate continuous use, rubbing of nose, etc. • Compliance all the infection prevention measure - hand washing is not routinely performed - wrong order in self-decontamination on leaving the infection ward - performing high risk procedure without full protection • 9. Long exposure time of the nursing staff to the infected patients • 10. Social contact with “infected” colleague with early (mild) symptoms such as tea break, dinning together, sharing room • tea break was held in the pantry within the infected ward area • 11. Short posting of staff into infected area • -HCW drafted into an infection ward for 1 day
Patient issues 12. Patient not wearing mask. 13. Possible contamination by patient (saliva, food, etc) during feeding, medication round, etc.
ACTION PLAN: • 1. To establish an “Infection risk and safety” • concept and culture across NTEC- commenced Saturday 29th March 2002 across NTEC • 2. Re-classification of level of “risk” of the wards and • to ensure appropriate barrier protective apparel • for all staffs, patients and visiting relatives (i) Ultra-high risk wards • (ii) High risk wards • (iii) Moderate risk wards • Structured briefing and training on caring • for patients with SARS- compulsory for staff going to work in the infection wards.
Staff protection • (i) Appropriate barrier protective apparel (ii) Ensure the mask (N95) fit well for ultra high risk staff • (iii) Proper barrierprotective process [入門七事, 出門七事](iv) Enforce hand washing / disinfection • 5. Staff compliance(i) Safety controller (SC) to be on duty on each shift • (ii) SC to undergo proper instruction course • (iii) Remind all the staff of the IC measure before each shift. • Patient compliance(i) Ensure all patients wear mask all the time (ii) prohibit patient touching the case note, x-ray etc • Use of Nebuliser Prohibited
8. Management issues / contingency plan(i) Establish rapid surveillance system (a) surveillance team to closely monitor any outbreak (b) rapid analysis of the reason for the outbreak • (ii) Establish rapid response plan for outbreak of infection Be prepared for sudden major outbreak • (i) designated stand-by ward (preferably with isolation facility)(ii) identify trained standby staff (doctor, nurse, AH, HCA) (iii) protective apparels to be made available immediately.(iv) defined action plan (v) establish control centre • By Dr. SF Lui / Dr. Donald Lyon • for Infection Control Unit of PWH • and NTEC Committees for Risk Management and Quality Assurance • 6 April 2003
HAHO IC ENFORCEMENT TEAM HOSPITAL IC ENFORCEMENT TEAM DEPARTMENT IC ENFORCEMENT TEAM WORK UNIT IC ENFORCEMENT TEAM
NTEC SARS PREVENTION TEAM IC officer IC unit staff RM staff SARS Data manager HOSPITAL SARS PREVENTION TEAM IC officer IC unit staff RM staff SARS Data manager DEPARTMENT SARS PREVENTION TEAM D - ICO WARD / UNIT / OFFICE SARS PREVENTION TEAM U - ICO
Role of Unit ICO To coordinate the IC programs at ward / unit / office level (1) To conduct environmental risk scanning (for cross-infection) (2) To verify the risk level (stratification) with the DICOif necessary, to add additional specific IC guideline for the unit (3) To ensure the appropriate IC program - ensure the IC program is implemented on the department / ward level - appoint shift ICO- ensure all staff have attended briefing on prevention of SARS- ensure there is briefing on IC control for every shift (4) to report suspected case to DICO (5) To conduct regular random audit(6) To monitor the health status of the staff on the ward / unit / office - ensure staff with febrile illness or symptoms of SARS are refrained from work and advised to seek medical treatment (7) To monitor the health status of the patient in particular, signs and symptoms of febrile illness
CONFIRMED CASE OF SARS OF HCWs AT PWH Phase 1 Phase 2 Phase 3 Phase 4 Phase 5 Phase 6 N = 73 N = 40 N = 0 N = 16 N = 0 N = 4 Nebuliser (6-14/3) Barrier-Man, Extraction Fan (17/4) Extra IC measure (27/3) Close A&E (19/3) open A&E (30/3) Readmit Patient (6/4)
PROBLEMS / ISSUES (1): • (1) ENVIRONMENTAL- ward layout, airflow, bedpan washer, etc • (2) PATIENT • Atypical presentation (especially elderly patient) - Multiple diagnosis / infection> Need high level of awareness / suspicion • Unsuspected AP admitted or developed on the ward • > reorganize the ward / cohort patients with fever • Triage / isolation system • confirmed AP / SARS ward • (b) suspected SARS ward • (c) infection triage / fever ward • (d) Other ward
Problems / issues (2) (3) CARING OF PATIENTElderly patient, need nursing care, close contact ++, Handling of excreta, contact with saliva, vomitus High risk procedures > Strict IC prevention measures (4) CROSS INFECTIONpatient-staff, staff-staff, staff-patient, patient-patient (staff continue to work with symptoms) > Strict IC measures on the ward > take immediate sick leave when develop symptom (fever) (5) Staff issues- Adequate training / preparation - Adequate & appropriate protection (PPE)
互相關懷,互相支持,互相監察 口罩眼鏡頭帽擋飛沫 外袍護手鞋套防病毒 返回程序除裝備 護理前後要洗手 保護措施必遵行 戰勝病毒人人責 守紀律 依程序 防病毒 停擴散
Action plan: 1. Establish NTEC SARS prevention team 2. Establish NTEC SARS infection control and prevention program== > implementation at department / ward / unit / office level== > monitoring and auditing at department / ward / unit / office level(The IC program must be established and implemented on every ward / unit / office within NTEC) 3. Appointment of Hospital Infection Control Officer==> Appointment of Department Infection Control Officer==> Appointment of Unit Infection Control Officer(With on-duty Infection Control Officer for each shift)
Role of Hospital ICO To coordinate the IC programs at hospital level (1) To ensure each department has appointed a department ICO to implement the IC programs (2) To ensure the IC programs are implemented across the hospital (3) To conduct regular random audit (4) To ensure the IC control protocols are being followed within the hospital(a) identification and reporting of suspected SARS case (b) Policy for general ward after the identification of a patient or staff suspected / confirmed as a case of SARS.
Role of Department ICO • To coordinate the IC programs at department level • To ensure each ward / unit / office has appointed a Unit ICO (UICO) • To ensure all UICOs have attended briefing session on NTE SARS Prevention program • (3) To ensure the IC programs are implemented on the ward level- to agree with the UICO on the appropriate risk level for the unit- to agree with the UCIO on additional / specific guidelines for the unit • (4) To ensure the IC control protocols are being followed within the hospital(a) identification and reporting of suspected SARS case (b) Policy for general ward after the identification suspected case of SARS • (5) Establish channel of communication - between H-ICO, D-ICO and U-ICO • - With Hospital SARS Data manager • (6) To conduct regular random audit