Download
1 / 39
410 likes | 737 Views
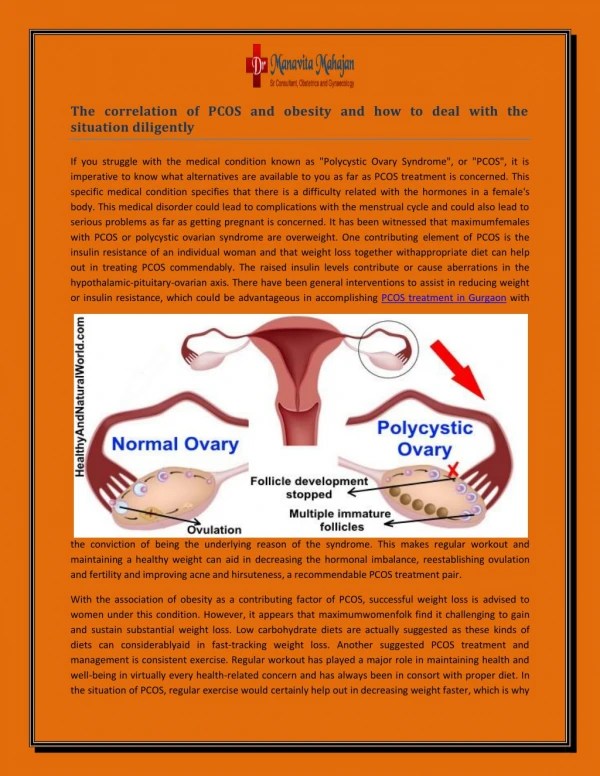
Lifestyle Therapy and Fertility in Women with PCOS. Infertility Treatment in PCOS. Richard S. Legro, M.D. Penn State College of Medicine Dept of Ob/Gyn Hershey, PA USA.

E N D
Lifestyle Therapy and Fertility in Women with PCOS Infertility Treatment in PCOS Richard S. Legro, M.D. Penn State College of Medicine Dept of Ob/Gyn Hershey, PA USA
AUTHORS' CONCLUSIONS: No RCTs were located that assessed the effects of preconception advice on the chance of a live birth or other fertility outcomes in people who perceived that they may be infertile and were investigating the possibility of medical treatment to address subfertility.
There ıs no evidence based schema Hum Reprod. 2008 Mar;23(3):462-77 and Fertil Steril. 2008 Mar;89(3):505-22
First Line Treatment Options Hum Reprod. 2008 Mar;23(3):462-77 and Fertil Steril. 2008 Mar;89(3):505-22
Can we achieve meaningful weight loss which will improve fertility outcomes?
Limitations of Lifestyle Therapy in Infertility • Dose? • Is there an ideal rate of weight loss or activity increase • Duration? • How long should the intervention be instituted • Timing? • Is the intervention before or during infertility treatment? • Patient Compliance (buy in) • Will patients be able to follow our instructions
RCT of Lifestyle vs Medicine in PCOS (?6 mos) N = 343 women Lifestyle: 500 Kcal daily diet deficit, 3-5x week exercise x 30 mins, had to lose 5% of body weight to be in the study!! P = 0.56 Karimzedah, Fertil Steril, In Press
Change in BMI with Lifestyle in PCOS (+/- metformin) Tang et al, Hum Reprod 2006
Metformin, Lifestyle Modification or OC treatment in PCOS Pilot trial of 43 obese adolescents with PCOS randomized to metformin, placebo, lifestyle modification or oral contraceptive for 6 months Lifestyle Modification: Combined group start, parent/adolescent 24 class educational session, 500 cal/d deficit, 30 mins/d moderate to intense activity, unmonitored) 9 dropped out ( 3 of 11 in lifestyle) Hoeger, et al JCEM 2008
Weight changes by group Hoeger, et al JCEM 2008
Combination therapy for obese PCOS adolescents Follow Up Trial of 36 obese adolescents treated with oral contraceptive (ethinyl estradiol + drosperinone) with metformin or placebo 4 dropped out over the 6 month trial. All received lifestyle modification program as before (parent/adolescent educational program, 500 cal/d deficit/30 mins/d exercise- now monitored, flexible enrollment, email/web support) Hoeger et al JCEM 2008
Reduction in Weight over 24 weeks P<0.01 P<0.01 NS Hoeger et al JCEM 2008
High Dropout in PCOS Lifestyle Studies 50% Dropout after Randomization Thomson, R. L. et al. J Clin Endocrinol Metab 2008;93:3373-3380
Weight loss (%) Over 20 Weeks by treatment group Thomson, R. L. et al. J Clin Endocrinol Metab 2008;93:3373-3380
Adults and Adolescents Consented and Screened (n=215) Randomized (n=136) Exclusions (n=79) • Reasons for Exclusion: • Ineligible (n=25) • Withdrawn consent (n=24) • Lost to follow-up (n=30) Metformin (n=66) Placebo (n=70) Dropout (n=34) Dropout (n=46) • Reasons for Dropout: • Medication side effects (n=6) • Lost interest/unable to comply (n=4) • Personal constraints/health issues (n=8) • Lost to follow-up (n=16) • Reasons for Dropout: • Lost interest/unable to comply (n=10) • Personal constraints/health issues (n=13) • Pregnancy (n=4) • Lost to follow-up (n=19)
Penn State Rural Primarily Caucasian Located in Hershey PA Meharry Urban Diverse Located in Nashville TN Penn State College of Medicine/ Meharry Medical College Demographics
Dietary Lose 7% of body weight in 6 mos and maintain. Hypocaloric diet Exercise Supervised 1 session/week Unsupervised 1500-2000 kcal/wk Monitor Submaximal VO2 Max monthly Lifestyle Intervention
Best Short Term and Long Term Weight Loss with a Low Carbohydrate Diet Shai I et al. N Engl J Med 2008;359:229-241
Summary: Lessons Learned • External Validity • Many will not even attempt a lifestyle intervention • Most who do will drop out • Severely obese patients may be poor candidates for such programs • There will be hurdles to implementing these programs in our current medical system • Best Case Scenario • Modest Effects, ? Improved outcomes
The common resources of the lancet, a garden, a kitchen, fresh air, cool water and exercise will be sufficient to cure all diseases that are at present under the power of medicine Benjamin Rush (1745-1813)
Weight Changes among Subjects in the Swedish Obesity Study over a 10-Year Period Sjostrom, L. et al. N Engl J Med 2004
Unadjusted Cumulative Mortality After Bariatric Surgery Sjostrom L et al. N Engl J Med 2007;357:741-752
NIH consensus: Indications for Bariatric Surgery • BMI > 40 • BMI > 35 with serious medical comorbidities • Is PCOS and/or infertility a serious medical comorbidity Malcolm, NEJM, 2009
Reproductive Health in Women undergoing Bariatric Surgery • 1,538 females having bariatric surgery (NIH-LABS Consortium). • PCOS had been diagnosed in 13.1% of subjects. • Women who were obese by 18 years old were more likely to report PCOS and infertility and less likely to have ever been pregnant, compared with women who became obese later in life. • Future pregnancy was important to 30.3% of women younger than 45 years, and overall to 51.4%. Gosman et al, Fertil Steril, 2009
Clinical and biochemical characteristics of the morbidly obese PCOS patients submitted to bariatric surgery, before and after weight loss Escobar-Morreale, H. F. et al. JCEM 2005
Conclusion: Rates of many adverse maternal and neonatal outcomes may be lower in women who become pregnant after having had bariatric surgery compared with rates in pregnant women who are obese; however, further data are needed from rigorously designed studies.
Can we achieve meaningful weight loss which will improve fertility outcomes? Only with bariatric surgery!
Supported by NIH grants, K08 and K24 grant, The National Cooperative Program for Infertility Research U54 HD 34449, U10 38992, Reproductive Medicine Network, 1R01HD056510 and A General Clinical Research Center grant MO1 RR 10732 to Penn State Northwestern Andrea Dunaif, M.D. Virginia Commonwealth Jerry Strauss, M.D.,Ph.D., John Nestler, M.D. University of Pennsylvania Christos Coutifaris, M.D., Ph.D. Rich Spielman, Ph.D. Anuja Dokras, M.D., Ph.D. Penn State- Jan McAllister, Ph.D. Larry Demers, Ph.D. Bill Dodson, M.D. Rich Zaino, M.D. Peter Lee, M.D., Ph.D. Alex Vgontzas, M.D. Allen Kunselman Jami Ober Kelly Stamets Rawa Patsy Emily George Sandra Eyer RMN Principal Investigators Funding/Collaborators
OCP vs Weight Loss for Pregnancy in Polycystic Ovary Syndrome OWL-PCOS