Download
1 / 38
450 likes | 823 Views
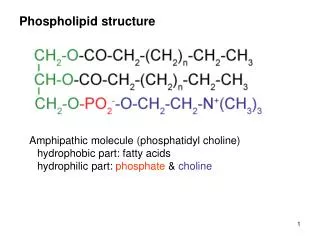
Anti- phospholipid Antibody Syndrome. Dr Ramesh Jois Consultant Rheumatologist Fortis Hospital & Kanva Diagnostics. History. Conley (1952): Unusual clotting inhibitor causing hemorrhage in SLE. (Lupus anticoagulant, BFP-STS) Bowie (1963): Paradoxically had thrombosis.

E N D
Anti-phospholipidAntibody Syndrome Dr RameshJois Consultant Rheumatologist Fortis Hospital & Kanva Diagnostics
History • Conley (1952): Unusual clotting inhibitor causing hemorrhage in SLE. (Lupus anticoagulant, BFP-STS) • Bowie (1963): Paradoxically had thrombosis. • Johansson (1977):”syndrome” of recurrent thrombosis associated with LAC. • Nilsson (1975): Recurrent spontaneous abortion might be associated with LAC. • Carreras(1981): LAC + Recurrent fetal loss + Thrombosis • Harris (1983): Solid phase anti-cardiolipin assay. • McNeill (1990): APL Ab bind diverse protein’s: β2GP-1, prothrombin (Galli 1990) & phospholipids (Pierangelli 1996). • Wilson (1999): Classification criteria for APLS.
APLA Primary Secondary Systemic Lupus Erythematosus. Rheumatoid arthritis Scleroderma Polymyositis Sjogren’s
APLA Classification Criteria 1. Thrombosis • Arterial - Stroke / TIA commonly. Rare: Retinal artery/ Mesenteric/ Coronary/ Pulmonary/ Extremities. • Venous - DVT/ Central Venous Sinus/ Pulmonary / Retinal Vein/ Superficial Veins/ Unusual site (Axillary, Hepatic, Renal, IVC etc) • Small vessel – Digital gangrene, Leg ulcers.
APLA Classification Criteria 2.Pregnancy outcomes • One or more late-term (>10wks) spontaneous abortion. • Three or more unexplained, consecutive, spontaneous abortions before 10 weeks gestation. • One or more premature births of a morphologically healthy neonate at or before 34 weeks’ gestation because of severe pre-eclampsia or eclampsia or severe placental insufficiency.
APLA Classification Criteria 3. Laboratory criteria • Positive: (1) Lupus Anticoagulant (2) Moderate to high levels of IgG or IgM anti-cardiolipin antibody (>40GPL/MPL or higher than 99th percentile) or (3) Anti–β2 glycoprotein 1 on at least two occasions at least 12 weeks apart. One clinical + one lab criterion = Definite APLS (Classification criteria) Miyakis et al. J Thromb Haemost.2006;4:295-306
Anti-phospholipid Antibody • LAC most powerful predictor of thrombosis (40-fold increased risk of stroke, 5-fold for MI & increased risk for recurrent miscarriage before 24 weeks) ¹ ² • LAC –ve APLA +ve : Increased risk of thrombosis & miscarriage (lesser than LAC +)² • Anti β2 GP-1: Negative association in 3 systematic reviews. Doubled risk for stroke and not MI¹. • Triple antibody +ve: Highest risk for arterial / venous thrombosis and obstetric events³ 1.Urbanus et al.LancetNeurol 2009;8:998-1005 2.Opatrny et al.JRheumatol 2006;33:2214-21 3.Ruffati et al.Arth Care Res.2010;62:302-07
Anti-phospholipid Antibody • APLA +ve in 30-40% patients with SLE but less than 40% develop thrombosis¹. • APLA +ve in 1 in 5 patients with stroke in patients < 50yrs². • DVT with no SLE: APLA +ve in 24% and LA in 4%³ • 10-15% of women with recurrent miscarriage are APLA +ve⁴. • APLA +ve in 11-29% of women with PET (compared to 7% in controls)⁵ • Population-based study : APLA +vity increased risk of PET (OR 2.9) & placental insufficiency (OR 4.58)⁵ • Obstetric APLA: high risk for subsequent thrombotic events. • 5% healthy individuals are positive for APLA. Clinical risk for thrombosis is not known. Mok et al.Arth Rheum 2005;52:2774-82 3. Roldan et al.Thromb Res 2009;124:174-77 Bushnell et al.Stroke 2000;31:3067-78 4. Rai et al.HumanReprod. 1995;10:2001-05 5. Clark et al.CurrRheumatol Rep 2007;9:219-25
Marchetti et al. Clinical and Developmental Immunology Volume 2013, Article ID 159124, 9 pages http://dx.doi.org/10.1155/2013/159124 7% 28% 11% “EURO- PHOSPHOLIPID” PROJECT
Other clinical features • Thrombocytopenia, Hemolytic anemia (DCT +ve). • Livedoreticularis (25%) – high risk for arterial thrombosis. • Cardiac valve disease - MV > AV, MR > MS, Asymptomatic. • Nephropathy – Thrombotic microangiopathy (HT, non-nephroticproteinuria, renal impairment). • Neurologic manifestations: Myelopathy, Chorea, Epilepsy, Migraine, Cognitive impairment (MR white-matter lesions).
Catastrophic APLA • Rare. Widespread small-vessel thrombosis, multi-organ failure, high mortality. 1. 3 organ/ system involvement 2. Simultaneous/ within a week 3. HPE: small vessel occlusion 4. LAC/ aCL + twice 6 wks apart • Definitive : all 4 criteria • Probable: criteria 1,2,4 / criteria 1,3,4 All criteria but 2 organ involvement All criteria but LAC/ aCL tested DD: TTP, DIC Buciarelii et al. Arth Rheum. 2006;54(8):2568-76 Asherson RA. Medicine (Baltimore).1998;77(3):195-207
Inflammation Ruiz-Irastorza et al. The Lancet,376, 9751, 1498 – 1509, October 2010
Modifiable riskfactors: HT, Smoking, Cholesterol, OCP
Prevention of recurrent thrombosis – Secondary Thromboprophylaxis • Recurrent thrombosis occurs in about 69% over 10 years of observation. • Recurrences can be prevented by oral anticoagulation. • Intensity of anticoagulation is still a matter of debate. INR 2-3 Vs 3-4. • High dose steroid + anticoagulation for less severe catastrophic APS. • IVIg plus plasmapheresis in addition for severe cases.
Secondary Thromboprophylaxis • Ruiz-Irartoza et al. Systematic review ¹: • First venous event: Risk of recurrence significantly reduced with INR 2-3. • Arterial or recurrent thrombotic event or both: risk of recurrence high with INR 2-3; infrequent recurrence when INR 3-4. 1.Ruiz-Irartoza et al.Arth Rheum 2007;57:1487-95
Recommendations • Definite APLA: indefinite anticoagulation - first venous event: INR 2-3 • first arterial event: INR 3-4 or combined antithrombotic treatment with INR 2-3. • Recurrent event despite warfarin (INR 2-3): INR 3-4 • Single +ve test / Low-titre APLA (especially with reversible triggers): • First venous event: as per standard DVT protocol(3-6m) • First arterial event: as per standard recommendations 1.Ruiz-Irartoza et al.13th International Congress on APLA. Lupus 2011; 20: 206
Primary prophylaxis • Still contentious! - Asymptomatic carriers. - SLE with antibody positivity. - Obstetric APLA. • Reduction of other risk factors for thrombosis. • Cover high risk situations- surgery, postpartum, long lasting immobilization etc. (thromboprophylaxis) • HCQS + Low dose aspirin – SLE with +ve antibody. • Low dose aspirin or no therapy – Obstetric APLA • No therapy – Asymptomatic carriers of APLA
Obstetric APLA • Planned pregnancy. • Complete antibody profile. • Screen for LUPUS. • Frequent antenatal visits. • Moniter for PET - HTN, Proteinuria etc. • Fetal surveillance (placental insufficiency) to begin at 32 wks or earlier and continue every week until delivery. • Uterine and umbilical artery doppler to assess the risk for PET, Placental insufficiency, Fetal growth restriction. - After 20th week of gestation; Normal value have high negative predictive value.
Obstetric APLA • Heparin started only after confirmation of pregnancy on ultrasonography. • Pre-conceptional Aspirin – helpful for implantation. • Warfarin – Teratogenic, avoided between 6-12 weeks. • Steroids – No role. • IVIg – No role (Pregnancy loss Study Group¹). 1. Am J Obstet Gynecol. 2000 Jan;182(1 Pt 1):122-
Obstetric APLA without Thrombosis • Recurrent Early (pre / embryonic) miscarriage: - Aspirin alone or together with LMWH (prophylactic dose). • Fetal death (>10 wks) or previous early delivery (< 34 wks) due to PET or placental insufficiency: - Aspirin plus LMWH (prophylactic dose)
Obstetric APLA with previous thrombosis • Aspirin plus LMWH (therapeutic dose) Eg: Enoxaparin 1mg/kg sc 12 hrly Daltaparin 100U/kg sc 12 hrly • Monitoring difficult - ?Anti-Factor Xa activity.
Does combined prednisolone and low molecular weight heparin have a role in unexplained implantation failure? • A combination of oral prednisolone and low molecular weight heparin may have a significant effect on pregnancy and implantation rates in prior unexplained, failed implantation. Fawzy M. Arch Gynecol Obstet. 2013 Sep 19. [Epub ahead of print]
HCQS – An old friend with a new role? • Reduce anti-phospholipid titers in the plasma of patients with persistent aPL. • Improve fetal outcomes in SLE treated pregnant patients. • Reduces the binding of anti𝛽2GP1 Abs at the surface of trophoblastic cells. • Restore the expression of annexin, preventing pathological activation of trophoblastic cells. Clinical and Developmental Immunology. Volume 2013, Article ID 159124, http://dx.doi.org/10.1155/2013/159124
Future Therapies • Combination anti-aggregant therapy (aspirin + clopidogrel or dipyridamole): especially when warfarin is contraindicated. • Oral anti-factor Xa drugs (rivaroxaban, apixaban) - As effective as warfarin. • Direct thrombin inhibitors (dabigatran) - RE-LY trail (AF), RECOVER trial (DVT) • Statins (fluvastatin, rosuvastatin) • Inhibhition of tissue factor production by APLA • Prevent increased adhesiveness of endothelial cell by antiβ2 • Decreased risk of DVT in healthy people with normal cholesterol (JUPITER)
Summary • APLA is an important cause of thrombosis and recurrent pregnancy loss. • Anticoagulation should be evidence-based. • Therapy should be individualized. • Asymptomatic carriers do not need therapy. • Combined care with Rheumatologist / Hematologist improves obstetric outcome.
Obstetric APLA - Postpartum • With previous thrombosis: - Switch to warfarin when clinically stable. • Without previous thrombosis: - LMWH (prophylactic dose) for 4-6 weeks or warfarin. • Heparin and warfarin – safe for breastfeeding mothers.
Prevention of pregnancy loss • No h/o thrombosis/miscarriage-observation/ low dose aspirin. • Recurrent early miscarriage- low dose aspirin • Previous thrombosis- aspirin+ LMW heparin. • Late foetal loss/ failure of aspirin- LMW heparin+ aspirin. • Cover post partum period • Close foetal monitoring and timely delivery-improves foetal survival. • Both warfarin and heparin are compatible with breast feeding.
Variants • HELLP Syndrome: Haemolysis, Elevated liver enzymes, Low platelets in women with PET and positive APLA. • EVANS Syndrome: Haemolysis with thrombocytopenia.
Pathogenesis • Defect in cellular apoptosis---exposes membrane phospholipids---binds antibody. • Oxidized β2GP1---Dendritic cell activation---production of autoantibodies. • Antibodies against prothrombin, Pr C /S. • Monocyte, Platelet & Endothelial cell activation. • Complement activation (pregnancy loss)
Pathogenesis • Anticardiolipin antibody: against membrane anionic phospholipids. • Anti-β2 GP1: Apo-lipoprotein H (β2glycoprotein) antibodies against domain 1 of β2. • Lupus anticoagulant: Circulating anticoagulant
Future Therapies • Hydroxychloroquine • Reduction of thrombosis & cardiovascular deaths. • Platelet activation and clotting inhibition. • Directly inhibits the binding of antiphospholipid antibody-β2-glycoprotein-1 complexes to phospholipid surfaces. - Protective effect of the annexin A5 shield formed over phospholipidbilayers from damage induced by APLA in pregnancy. • B-cell depletion (rituximab) – case reports in severe disease.