Download
1 / 55
580 likes | 1.24k Views
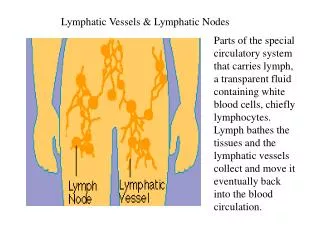
Pathology of blood and lymphatic vessels. Pathology of blood and lymphatic vessels. The main cellular components of the walls of vessels are: 1) endothelial cells 2) smooth muscle cells 3) pericytes (the cells normally arranged along capillaries and venules).

E N D
Pathology of blood and lymphatic vessels The main cellular components of the walls of vessels are: 1) endothelial cells 2) smooth muscle cells 3) pericytes (the cells normallyarranged along capillaries and venules)
Pathology of blood and lymphatic vessels • Endothelial cells: • a)serve as a semipermeable membrane, • b) regulate thrombosis, thrombolysis and platelet adherence, • c) influate vascular tone and blood flow, • d) metabolize hormones, • e) regulate immune and inflammatory reactions, • f) modify lipoptoteins in the artery wall, • g)regulate the growth of other cell types, including smooth muscle cells.
Pathology of blood and lymphatic vessels Endothelial injury is critical to the formation of thrombi, to the initiation of atherosclerosis and the vascular effects of hypertension and other disorders !!
Pathology of blood and lymphatic vessels • Endothelial dysfunction • Endothelial activation
Pathology of blood and lymphatic vessels The term endothelial dysfunction is often used to describe several types of potentially reversible changes in the functional state of endothelial cells that occur in response to environmental stimuli.
Pathology of blood and lymphatic vessels The term endothelial activation reflects alterations in gene expression and protein synthesis. Inducers of endothelial activation include cytokines and bacterial products (which cause inflammatory injury and septic shock), hemodynamic stress and lipid products (involved in pathogenesis of atherosclerosis), advanced glycosylation of end products (involved in pathogenesis of diabetes), as well as viruses, complement components and hypoxia. Activated endothelial cells also elaborate adhesion molecules, other cytokines and chemokines, growth factors, molecules of the major histocompatibility complex (MHC), procoagulant or anticoagulant factors and vasoactive molecules that are involved either in vasoconstriction or in vasodilatation.
Pathology of blood and lymphatic vessels 2)Smooth muscle cells are capable: a)to mediate vasoconstriction, b) to mediate vasodilatation, c) to synthesize the collagen, elastin, and proteoglycans, d) to elaborate the growth factors and cytokines, e) to proliferate, and f) to migrate to the intima. 3) Pericytes have role as supportive and connective elements.
Pathology of blood and lymphatic vessels The final result of vascular injury is intimal thickening !!
Vascular Diseases Diseases of arteries Diseases of veins and lymphatics Tumors
Diseases of arterias A) Congenital anomalies B) Atherosclerosis C) Hypertensive vascular disease D) Inflammatory disease – Arteritides (Vasculitides) E) Raynaud disease F) Aneurysms a dissections
Diseases of arterias A. Congenital Anomalies Aberrations of the usual anatomic pattern of branching, shape and anastomosing. Importance have only: berry aneurysms (developmental aneurysms involving cerebral vessels) and arteriovenous fistulas or aneurysms (abnormal communications between arteries and veins usually arised as developmental deffect, from rupture of an arterial aneurysm into adjacent vein, or from injury, or from inflammatory necrosis of adjacent vessels). Their clinical significance depends on short-circuit blood from the arterial to the venous side, causing the heart to pump additional volume, sometimes inducing cardiac failure.
Diseases of arterias B. Atherosclerosis It is a generic term for three patters of vascular disease that have in common thickening and loss of elasticity of arterial walls: 1)Atherosclerosis– characterized by the formation of intimal fibrous plaques that often have a central core rich in lipid (fibrofatty plaques). 2) Mönckeberg medial calcific sclerosis – characterized by calcific deposits in medium-sized muscular arteries in persons older than 50 years. These medial lesions forming irregular medial plates or discrete transverse rings have much less clinical importance. 3) Arteriosclerosis – the hyaline and hyperplastic thickening of small arteries and arterioles which causes luminal narrowing and down stream ischemic injury.
Diseases of arterias B. Atherosclerosis Introduction • Atherosclerosis significantly contributes to serious morbidity and mortality – approximately half or more of all deaths. • It primarily affects elastic arteries (e.g., aorta, carotid and iliac arteries) and large and medium sized muscular arteries (e.g., coronary and popliteal arteries). • The disease often begins in childhood, but symptoms are not usually evident until middle age. • Symptomatic atherosclerotic disease is most often localized to the arteries supplying the heart, brain, kidneys, lower extremities, and small intestine. • Myocardial infarction (heart attack), cerebral infarction (stroke), and aortic aneurysms are the major consequences of this disease. • There are also other important consequences such as gangrene of the legs, mesenteric occlusions, sudden cardiac death, chronic ischemic heart disease, and ischemic encephalopathy.
Diseases of arterias B. Atherosclerosis Morphology The key processes are intimal thickening and lipid accumulation, producing the characteristic atheromatous plaques (AP). Their precursors are fatty dots (FD) and streaks (FS).
Diseases of arterias B. Atherosclerosis Fatty streaks present nearly universally in children. They do not cause any disturbance in blood flow, however, they may be precursors of AP. FSs begin as multiple yellow flat spots – fatty dots (FD) which are less than 1 mm in diameter. Subsequently they merge into elongated (1 cm long and longer) FSs. They are composed of lipid-filled foam cells with T-lymphocytes and extracellular lipids.
Diseases of arterias B. Atherosclerosis Atheromatous plaques are the basic lesions within the intima, having a core of lipid (mainly cholesterol and cholesterol esters) and a covering fibrous cap. APs are also called fibrous, fibrofatty, lipid, or fibrolipid plaques which have white to whitish yellow colour and rise intima slightly into the lumen of the artery. The centers of larger plaques may contain a yellow debris, hence the term atheroma. Their distribution in humans is characteristic. The abdominal aorta is usually much more involved than thoracic aorta, and aortic lesions tend to be much more prominent around the origins (ostia) of its major vessel branches.
Diseases of arterias B. Atherosclerosis Atheromatous plaques have 3 principal components: 1) cells, including smooth muscle calls, macrophages, and other leukocytes, 2) connective tissue extracellular matrix, including collagen, elastic fibers, and proteoglycans, and 3) intracellular and extracellular lipid deposits. In advanced atherosclerosis, the fatty atheroma may be converted to a fibrous scar.
Diseases of arterias B. Atherosclerosis The complicated lesions are defined by: a) patchy or massive calcification, b) focal rupture or gross ulceration, c) thrombus formation (thrombosis) producing emboli, d) hemorrhage into a plaque, e) aneurysmal dilatation of large vessels.
Diseases of arterias B. Atherosclerosis Epidemiology Atherosclerosis is virtually ubiquitous among the populations of North America, Europe, Australia, New Zealend, Russia. In contrast, it is much less prevalent in Central and South America, Africa, and Asia. Many evidences exist that it depends on the life style and dietary customs.
Diseases of arterias • B. Atherosclerosis • Risk Factors • Age (advanced age), sex (male, postmenopausal women, the protective effect of estrogens), genetics (polygenic familiar predisposition, genetic abberrations in lipoprotein metabolism resulting in excessively high blood lipid levels), diet, life style, personal habit. There are 6 major well-accepted conditions such as: • hyperlipidemia, • hypertension, • smoking, • diabetes mellitus, • elevated plasma homocysteine, • factors affecting hemostasis and thrombosis.
Diseases ofv arterias B. Atherosclerosis Hyperlipidemia: It should be a major risk factor. Most of the evidences implicates hypercholesterolemia (hypertriglyceridemia is a less significant, but its effect may be greater in women than men). The major component of the total serum cholesterol is low-density lipoprotein (LDL) cholesterol. In contrast, there is an inverse relationship between symptomatic atherosclerosis and high-density lipoprotein (HDL) level. HDL is believed to mobilize cholesterol from existing atheroma and transport it to the liver for excretion in the bile (cholesterol bound to HDL is designated as the “good cholesterol“. The various classes of blood lipids are transported as lipoproteins complexed to specific apoproteins. They have many functions including activation and inhibition enzymes, facilitating transmembrane transport of certain lipoproteins, serving as ligands to high.affinity cellular receptors that guide the lipoproteins to specific sites of catabolism.
Diseases of arterias B. Atherosclerosis Hyperlipidemia:Dyslipoproteinemias result either from genetic mutations involving genes for apolipoproteins or from some other underlying disorder, such as the nephrotic syndrome, alcoholism, hypothyreoidism, or diabetes mellitus. Four types of lipoprotein abnormalities are frequently found in the population: 1) increased LDL cholesterol level, 2) decreased HDL cholesterol level, 3) increased chylomicron remnants and intermediate-density lipoproteins – IDL, 4) increased level of an abnormal lipoprotein Lp(a).
Diseases of arterias B. Atherosclerosis Hypertension: It is a stronger risk factor than hypercholesterolemia after age 45 years. Men whose blood pressure exceeds 169/90 mm Hg have a more than 5-fold greater risk of ischemic heart disease than those with blood pressures of 140/90 mm Hg or lower. Smoking:When one or more packs of cigarettes are smoked per day for several years, the death rate from ischemic heart disease increases twice. Diabetes mellitus: DM induces hypercholesterolemia and a markedly increases predisposition to atherosclerosis. The incidence of myocardial infarction is twice as high, the incidence of strokes is 4-fold greater, and the incidence of gangrene of the lower extremities 100-fold greater.
Diseases of arterias B. Atherosclerosis Elevated Plasma Homocysteine: Recent clinical and epidemiologic studies have indeed shown a more general relationship between total serum homocysteine levels and coronary artery disease, peripheral vascular disease, stroke, or venous thrombosis. There is evidence that homocysteine may cause endothelial dysfunction, through formation of reactive oxygen species. It also interferes with with the vasodilator and antithrombotic functions of nitric oxide. Factors Affecting Hemostasis and Thrombosis: Several other markers of hemostatic and thrombotic function are potent predictors of risk for major atherosclerotic events (plasminogen activator inhibitor-1 level, plasma fibrinogen level, C-reactive protein level).
Diseases of arterias B. Atherosclerosis Pathogenesis of atherosclerosis The contemporary view of the pathogenesis: Atherosclerosis is a chronic inflammatory response of arterial wall initiated by some form of endothelial injury!! There are described the following steps: a) chronic endothelial injury, b) insudation of lipoproteins (mainly LDL and VLDL) into the vessel wall, c) modification of such lipoproteins by oxidation, d) adhesion of blood monocytes to the endothelium, e) migration of monocytes into the intima and their transforamtion into macrophages and foam cells, f) adhesion of platelets to focal areas of denudation or to adherent leukocytes
Diseases of arterias B. Atherosclerosis Pathogenesis of atherosclerosis The contemporary view of the pathogenesis: Atherosclerosis is a chronic inflammatory response of arterial wall initiated by some form of endothelial injury!! Continuation: g) release of factors from activated platelets, macrophages or vascular cells, h) migration of smooth muscle cells from media into intima, i) proliferation of smooth muscle cells in the intima and elaboration of extracellular matrix, j) accumulation of collagen anf proteoglycans, k) enhanced accumulation of lipids within macrophages, smooth muscle cells and extracellularly.
Diseases of arterias C. Hypertensive Vascular Disease One of the most important risk factors in both coronary heart disease and cerebrovascular accidents. It may also lead to cardiac hypertrophy with heart failure, aortic dissectin, and renal failure. About 90-95% of hypertension is idiopathic and apparenly primary – essential hypertension. Of the remaining, 5-10% is secondary to renal disease or, less often, to narrowing of the renal artery (usually by an atheromatous plaque) – renovascular hypertension. Infrequently, secondary hypertension is the result of diseases related to the adrenal gland (such as primary aldosteronism, Cushing syndrome, pheochromocytoma etc.). About 5% of hypertensive persons show a rapidly rising blood pressure, which, if untreated, leads to death within 1 or 2 years – malignant hypertension.
Diseases of arterias C. Hypertensive Vascular Disease Morphology Hypertension accelerates atherogenesis and causes changes in the structure of the wall of blood vessels that potentiate both aortic dissection and cerebrovascular hemorrhage. In addition, hypertension is associated with 2 forms of small blood vessel disease – hyaline arteriolosclerosis (in elderly patients, more severe in patients with hypertesion and diabetes, a homogenous, pink, hyaline thickening of the walls of arterioles with narrowing of the lumen) and hyperplastic arteriolosclerosis(in patients with more severe elavation of blood pressure, there is typical onion-skin, concentric thickening of the walls of arterioles with progressive narrowing of the lumens).
Diseases of arterias D. Inflammatory Disease – Arteritides, Vasculitides Infectious Vasculitides: bacterial- Neisserial, Rickettsial, Spirochetal, fungal, viral, Non-Infectious Vasculitides: so-called systemic necrotizing vasculitides (affecting aorta, medium-sized vessels) and small vessel vasculitides (affecting arterioles, venules and capillaries). Pathogenesis involves immune compexes, antineutrophil cytoplasmic antibodies(ANCA) and antibodies to endothelial cells. Classification on the basis of the size of the involved blood vessels, the anatomic site, clinical manifestation and histological characteristics of the lesion:
Diseases of arterias D. Inflammatory Disease – Arteritides, Vasculitides Large Vessel Vasculitis Giant cell (temporal) arteritis: Granulomatous arteritis of the aorta and its major branches, with a predilection for extracranial branches of the carotid artery and the temporal artery. Usually occurs in patients older than 50 years and often is associated with polymyalgia rheumatica. Takayasu arteritis (pulseless disease): Granulomatous inflammation of the aorta and its major branches. Usually accurs in patients younger than 50 years.
Diseases of arterias D. Inflammatory Disease – Arteritides, Vasculitides Medium-Sized Vessel Vasculitis Polyarteritis nodosa: Necrotizing inflammation without glomerulonephritis or vasculitis in arterioles, capillaries, or venules. Kawasaki disease: Arteritis associated with mucocutaneous lymph node syndrome. Coronary arteries are often involved. Aorta and veins may be involved. Usually occurs in children. Thromoangitis obliterans (Buerger disease): Segmental, thrombosing acute and chronic inflammation of medium-sized and small arteries, principally the tibial artery in younger men who were heavy smokers.
Diseases of arterias D. Inflammatory Disease – Arteritides, Vasculitides Small Vessel Vasculitis Wegener granulomatosis: Granulomatous inflammation involving the respiratory tract and necrotizing vasculitis affecting capillaries, venules, arterioles and arteries. Necrotizing glomerulonephritis is common. Churg-Strauss syndrome:Eosinophil-rich and granulomatous inflammation involving the respiratory tract and necrotizing vasculitis affecting small and medium-sized vessels associated with asthma and blood eosinophilia. Microscopic polyangiitis: Necrotizing vasculitis with few or no immune deposits affecting small and medium-sized vessels. Necrotizing glomerulonephritis is common. Pulmonary capillaritis often occurs. Henoch-Schönlein purpura: Vasculitis with IgA-dominant immune deposits affecting small vessels. Typically involves skin, gut, and glomeruli. Associated with arthralgia or arthritis. Goodpasture syndrome: Glomerulitis and pneumonitis caused by anti-basement membrane of capillaries antibodies.
Diseases of arterias E. Raynaud Disease Paroxysmal pallor or cyanosis of the digits of the hands or feet and infrequently the tips of the nose or ears (acral parts) caused by intense vasospasm of local small arteries or arterioles. Typically in young, otherwise healthy women. No organic changes are present in the arterial walls except late, when intimal proliferation can appear.
Diseases of arterias F. Aneurysms and Dissection Aneurysm – localized abnormal dilatation of blood vessel that occurs most commonly in the aorta or the heart. It can be true (complete but often attenuated arterial wall components) or false (extravascular hematoma that communicates with the intravascular space). The 2 most important causes of true aortic (or any vessel) aneurysms are atherosclerosis and cystic medial degeneration. Typical is also syphilitic aneurysm (tertiary stage of syphilis).
Diseases of arterias F. Aneurysms and Dissection Aortic Dissection (Dissecting Hematoma) – is characterized by dissection of wall and penetration of blood in between and along the laminar planes of the media, with the formation of a blood-filled channel within the aortic wall – a dissecting intramural hematoma (aneurysm). It can rupture, causing massive hemorrhage. In contrast to atherosclerotic and syphilitic aneurysms, it is not usually associated with marked dilatation of the aorta. The more common and dangerous proximal lesions involving either the ascending postion of aorta only or both the ascending and the descending aorta are called types I and II of DeBakey´s classification (often called type A). Distal lesions not involving the ascending part of aorta and usually beginning distal to the subclavian artery are called DeBakey type III (type B).
Diseases of veins and lymphatics A) Varicose Veins B) Thrombophlebitis and Phlebothrombosis C) Syndrome of vena cava superior D) Syndrome of vena cava inferior E) Lymphangitis and Lymphedema
Diseases of veins and lymphatics A) Varicose Veins Abnormally dilated, tortuous veins produced by prolonged, increased intraluminal pressure and/or by loss of support of the vessel wall. Usually the superficial veins of the leg are involved. There is marked variation in the thickness of the wall. Intraluminal thrombosis and valvular deformities are frequently found. Despite thrombosis of superficial varicose veins, embolism is rare (sharp contrast to the relatively frequent thrombembolism that arises from thrombosed deep veins).
Diseases of veins and lymphatics There are two special sites of varix formation: Esophagus (in patients who have cirrhosis of the liver and portal hypertension, ruptura of an esophageal varix followed by hemorrhage may be very serious) and anorectal junction (varicose dilation of the hemorrhoidal plexus of veins called hemorrhoids resulting of prolonged pelvic congestion, source of bleeding and site of thrombosis).
Diseases of veins and lymphatics B) Thrombophlebitis and Phlebothrombosis Venous thrombosis caused by inflammation or by different mechanisms (hypercoagulability, immobilization, postoperative state, pregnancy etc.). The deep leg veins account for more than 90% of cases of thrombophlebitis. The venous thromboses have a tendency to embolization into lung.
Diseases of veins and lymphatics C) Syndrome of vena cava superior Usually caused by neoplasms (occasionally by other lesions such as aortic aneurysm) that compress or invade the v. cava superior (primary bronchogenic carcinoma, mediastinal lymphoma). The consequent obstruction produces a distinctive clinical complex (dusky cyanosis, marked dilation of the veins of the head, neck, and arms. Commonly the pulmonary vessels are also compressed, and consequently resipartory distress may develop.
Diseases of veins and lymphatics D) Syndrome of vena cava inferior This syndrome may be caused by the similar processes (hepatocellular carcinoma, renal cell carcinoma, thrombus). Obstruction induces marked edema of the legs, distention of the superficial collateral veins of the lower abdomen, and, when the renal veins are involved, massive proteinuria.