Download
1 / 37
370 likes | 528 Views
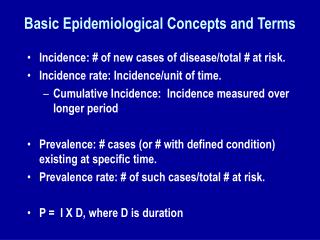
TB in a Low-Incidence State: Best Practices in New Hampshire. Presented by Judy Proctor, RN, BSN New Hampshire TB Program Coordinator May 14, 2007. Overview. New Hampshire (NH) TB Program model of care Common challenges in low-incidence states Building Partnerships Communication

E N D
TB in a Low-Incidence State: Best Practices in New Hampshire Presented by Judy Proctor, RN, BSN New Hampshire TB Program Coordinator May 14, 2007
Overview • New Hampshire (NH) TB Program model of care • Common challenges in low-incidence states • Building Partnerships • Communication • Training and Education • Standards of practice • Practical approaches in NH: snapshots to generate discussion
DANGERIn Low-Incidence Areas KEEP TB ON THE RADAR SCREEN
Snapshot of New Hampshire • Primarily rural, 10 counties • Population: 1,299,500 • 96% Caucasian • 4.4% Foreign-born • 1.7% Latino • 1.3% Asian • 0.7% Black/African American
New HampshireA Low TB Incidence State • Mean:17 cases annually over 15 yrs • Rate 1.3/100,000 • 78% FB, 2002 – 2006 • 85% in 3 SE counties since 2002 • 10 counties • 7 PH districts • 2 city health departments • LTBI reportable: high-risk group case management
New Hampshire TB Program A Centralized State Program • No county health departments • 2 large city health departments;contracts for services • Manchester • Nashua • Information flow is bi-directional • Nurse-case management/home-based model • Patients rarely hospitalized
NH TB Structure • No TB Clinics • No infrastructure for direct management of patients • Private providers diagnose & treat TB & LTBI • State doesn’t provide medications directly • Income eligibility • Cases usually referred to specialists for treatment: infectious disease or pulmonologists • Reliant upon other agencies for diagnosis/treatment: “THINK TB”
New Hampshire TB Staff • 2.4 State staff dedicated to TB • TB Nurse Manager • Part-time Training & Education Coordinator • Medical Secretary (vacant) • 7 State communicable disease public health nurses (PHNs) with geographic districts and competing priorities • 2 communicable disease epidemiologists
NH TB Staff • Medical consultants • State Epidemiologist & Deputy State Epidemiologist • 2 city Health Departments; nurse case management • Public Health Laboratory
NH TB Program Philosophy • Collaborative, community-centered approach • Public and private sector • “We need you; you need us”
“Successful patient and program outcomes rely upon close communication and collaboration of the public and private sector in TB prevention and control efforts.”
Common Challenges in Low-Incidence States • Partnership Building • Building personal community relationships • Communication • In-state: centralized • Training & education- maintain expertise • HR development funding • Implementing standards of practice • DOT
Building Partnerships • Regional PHN case manager outreach • Personal relationships over time • Program relies upon personal bonds to provide high-quality care • Visibility within the community • Based upon respect and trust • “Meet and greet” approach • Build bridges in the community
Building Personal Relationships/Partnerships • NHICEPs/board liaison • TB Medical Specialists • Home Health Agencies • Health-care Facility Licensing • Correctional Facilities • Lung Association of NH • Refugee Resettlement Agencies • Universities
Building Personal Relationships/Partnerships Getting to know your community • Who are the ICPs at facilities? Meet them & help them! • Which practices are knowledgeable and comfortable treating pts with TB? Meet & help. • Who is willing to learn? Help them. • What pharmacies stock TB medications? • Which HHA will accept Medicaid reimbursement? • Ask who knows the PHN in this community? • Who else needs to “THINK TB”?
Correctional Facility Example • Over years, PHN established relationship with county nursing home and jail through periodic disease investigations and outreach visits. • Impromptu meeting with jail Superintendent; discussed TB testing practices • Left business card
Correctional Facility Example • 2005: call from county jail about an inmate who might have TB • Inmate had been arrested 48 hours earlier after a car accident • Had been transported by officers to the hospital, the jail, the court, back to the jail • CXR now suspicious for TB • Plan: transport out of state • PANIC in the community- court, police, CF, hospital
Correctional Facility • Superintendent remembered and called PHN • Prompt interventions- Same day met with CF officers,sheriffs dept, police depts, jail leadership and medical staff • IC: AII cell, N-95 masks, sputum collection, transport protections • Able to defuse the situation quickly • Confirmation of TB
Human Resource Development Funding • 2005: new directive from CDC • HR development plan required • Target training of staff & providers • Who will do it? • Already wearing many hats • Reliant upon outside partners for care delivery- How to keep them informed and updated? • How to accomplish with limited resources?
HR Development Funding • Hired part-time (15 hours/week) TB focal point • Conducted provider/program training needs assessment in conjunction with evaluation project • modified survey tool from RTMCC to better meet needs in low-incidence state and included evaluation project • 1230 surveys mailed to select providers in 4 highest incidence counties • targeted specialty areas: family practice, internal medicine, pediatrics, ID and pulmonology • 398 responses received (32 % response rate)
HR Development Activities • Based on the provider survey data received • Developed TB training and HR development plan • Developed email list-serves for distribution of information and resources • i.e. Corrections, ICPs, IDs and Pulmonologists • Distribution of new products, guidelines and educational opportunities through list-serves • Annual TB conference focusing on areas of greatest provider need and interest • Plan: program brochure to better educate providers about our program and services
Education and Trainingof Program Staff • New employee orientation • On-going training • Staff case conference meetings every other month; training component included • Examples: New Diagnostics in TB, Refugee Health, XDR-TB, New guidelines • Weekly outbreak team meetings- teaching moment • Webinar trainings/tracking: encourage attendance • NHICEP meetings • Limited attendance at RTMCC,regional or national trainings
Health Care Provider Training • “THINK TB” message • Medical case consultation easily accessible • TB 101, DOT and TST workshops • Targeted annual TB conference in collaboration with local hospitals and NJRTMCC • Dartmouth Medical School residents on site • Brown bag presentations to medical resident training programs • Local, regional and national conferences • Webinars: New England TB Case series
Communication • Small size and centralized structure facilitates the mechanism of communication • Same people wear multiple hats • Meetings • Weekly and PRN Communicable Disease team meeting conference call • Every other month case conference with TB program updates and educational session • NHICEP state update every other month • Providers: THINK TB • Office visits: meet and greet, phone, email • Newsletter, annual report
Standards of Practice Universal Directly Observed Therapy (DOT)
Universal DOT • National recommendation • Administrative and TB Advisory Committee support: 1997 • Delivery model:Home Health Agencies (HHA) • Challenge to engage: • Program staff • Home Health Agencies (HHA) • Providers • Clients • Resulted in routine standard of practice
DOT • By PHN or HHA • Contract with HHA for DOT • Reimburse at current Medicaid rate • Train HHA staff: TB 101 With DOT • DOT letters for HHA • DOT Calendars • Monthly pill boxes • PHN maintains case management responsibilities • Incentives as needed- local grocery stores
TB in NH 1991-2005: DOT vs Self Administered Therapy 100% 90% 80% 70% 60% 50% Percentage 40% 30% 20% 10% 0% 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 Count Year No DOT Both 100% DOT
Summary of NH Strategies To Enhance TB Control Efforts • Regional PHN outreach • Market “THINK TB” message • Engage community in TB Control • Maintain internal and external TB training efforts • Ongoing communication between the public and private sector
Regional Efforts • Partnership, communication, standards of practice, E&T • Facilitated by Mark Lobato, CDC Regional Medical Officer • Periodic conference calls • NewEnglandTB.org • Genotyping workgroup • Training • Qtrly case series • Shared resources
New Hampshire TB Program • Phone: 603-271-4496 • Fax: 603-271-0545 • Email: Judy Proctor • Jproctor@dhhs.state.nh.us • Address: 29 Hazen Drive Concord, NH 03301
Acknowledgements • Lisa Roy, TB Education & Training Coordinator • NH Communicable Disease Control Staff • New England Regional TB Group • Jose T. Montero MD, State Epidemiologist • Elizabeth A.Talbot MD, Deputy State Epidemiologist and Assistant Professor Medicine at Dartmouth College