Download
1 / 41
460 likes | 1.39k Views
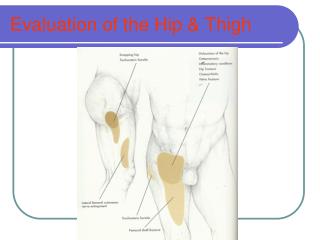
Evaluation of the Hip & Thigh. Hip & Thigh. Anatomy The hip is a multiaxial ball-and–socket joint that has maximum stability due to the deep insertion of the head of the femur into the acetabulum

E N D
Hip & Thigh • Anatomy • The hip is a multiaxial ball-and–socket joint that has maximum stability due to the deep insertion of the head of the femur into the acetabulum • The hip forms the critical link between the lower extremity and the trunk. Critical for ambulation, it has been described ad the “pivot upon which the body moves”.
Hip Joint • Articulations between the acetabulum of pelvis and head of femur • Ball and Socket joint • Femoral head is 2/3 of a sphere • Inside the acetabulum is a labrum • Synovial joint surround by strong lig. -Capsular lig. • Heavy musculature
Hip Joint • Inside the acetabalum of the glenoid labrum made of fibrocartilage and holds the head of femur in tight. • Acetabulum made up of the 3 bones of the pelvis together - ilium forms superior portion, inferior is the ischium and internal medially is the pubis • Synovial joint surrounded by strong ligaments. The whole attachment of the synovial lining is referred to as capsular ligament • Heavy musculature causes strong stability
Pelvic Girdle • 4 fused bones make up the girdle • 2 innominate bones, sacrum, and coccyx • Anterior articulation at the pubis symphysis • Posterior articulation at the sacrum and sacroiliac joint • Each innominate bone made up of 3 fused bones - ilium, ischium, pubis • Ilium forms the major portion of the iliac crest • ASIS - Anterior superior iliac crest • PSIS - Posterior superior iliac crest
Pelvic Girdle • Acetabulum • Has a labrum and fibrocartilage that holds the femoral head in tight • Synovial Joint • The whole attachment of the synovial lining is referred to as capsular lig. • Bursas • Iliopsoas bursa • Deep Trochanteric bursa
Active Motions of the Hip • Flexion – 110 to 122 degrees
Active Motions of the Hip • Extension: 17-25 degree
Active Motions of the Hip • Abduction: 35-40 degrees
Active Motions of the Hip • Adduction: 30 degrees
Active Motions of the Hip • Internal Rotation: 30-35 degrees
Active Motions of Hip Joint • External Rotation: 35- 40 degrees
Ligaments of Hip • Capsular Ligament • Intra capsular - fibers attached to rim of acetabulum and femur • Extra-Capsular Lig. • Iliofemoral Lig. • limits hip hypertension, ER, & Adduction • Pubofemoral Lig. • Prevents abduction and excessive ER
Ligaments of Hip • Extra-Capsular Lig. • Ischiofemoral Lig. • Prevents IR and adduction • Ligamentum Teres • Serves as vascular conductent for the medial and lateral circumflex arteries • May cause a disruption of these arteries
Femoral Triangle • Contains: • Inguinal ligament at upper border • Sartorius at lateral border • Adductor longus at medial border • Inside the triangle is the • Femoral artery • Femoral vein • Femoral nerve
Ossesous Deformities • Four common osseous deformities of the proximal femur are: • Coxa Vara • the angle between the ball and the shaft of the femur is reduced to less than 120 degrees. This results in the leg being shortened, and therefore a limp occurs • Coxa Valga • the angle formed between the head and neck of the femur and its shaft is increased, usually above 135 degrees. It is caused by a slipped epiphysis of the femoral head • Can occur as a primary problem or a sequela problem • Can occur unilateral or bilateral • Effects of osseous deformities are they can lead to alteration in wt. Bearing in the lower extremity and spine
Hip Joint Angle of Inclination • Femoral head is angled at 125 degree in frontal plane • This relationship of femoral head is known as the ANGLE OF INCLINATION and changes through a person’s development. • Slightly higher in women. • Increase in angle is Coxa Valga • Decrease in angle is Coxa Vara
Angle of inclination • An increase in the angle is referred to as coxa valga • A decrease in the angle is referred to as coxa vara • In either case the mechanical advantage of the gluteus medius is reduced by alternating its line of pull on the femur. • X-ray is necessary to determine angle accurately
Coxa Vara • Occurs when the angle between the femoral shaft and the femoral neck in the frontal plane (angle of inclination) is less than 125 degrees
Coxa Vara • Results in • Ipsilateral limb shortening which alters the biomechanics of the hip by shifting the wt. Bearing superiorly and laterally to the femoral head • The moment arm acting or the hip abductors is reduced resulting in weakness of the hip abductors • Anterior Pelvic Tilt
Coxa Vara • Developmental and acquired conditions resulting from Coxa Vara • Intertrochanteric fracture • Slipped Capital Femoral Epiphysis • Le-Calve-Perthes Disease • Congential Hip Dislocations
Coxa Vara • Clinical findings • A leg length difference • Gait abnormality associated with a Trendenleburg Gait • Hip abduction is restricted by the superior portion of the femoral neck or greater trochanter (Impingement) • Hip abductor muscle contractures occur • Pronated subtalar joint • Medial rotation of leg
Treatment for Coxa Vara • Treatment • Use of shoe lift to equalize leg lengths may be very helpful • Strengthening hip abductors • Avoid high impact sports
Coxa Valga • The angle between the femoral shaft and the femoral neck on the frontal plane is greater than approximately 125 degrees at skeletal maturation
Caused by • Ipsilateral limb lengthening resulting in a characteristics adducted posture of the lower limb. On wt. Bearing, the forces are shunted closer to the center of the head of the femur, which can cause hip dysplasia
Coxa Valga • Clinical findings of unilateral coxa valga include • Leg length difference, with the involved side being longer • Posterior pelvic tilt • With either bilateral or unilateral there is a gait abnormality associated with a + Trendelenburg sign • Lateral rotation of leg
Coxa Valga • Treatment • Similar to Coxa Vara • Shoe lift to equalize leg length • Strengthen hip abductors • Minimize prolonged standing and avoid high impact sports
Myotomes & Dermatomes • Myotomes • L1-L2 • Hip Flexion • L3 – Knee Extension • L4 Dorsiflexion • L5 Hallicus Extension • S1 • Hip extension & Plantar Flexion • S2 • Knee Flexion
Common Injuries • Contusions • Resulted from a direct blow ; most common site is the anterior lateral thigh • Myositis Ossificans • Abnormal ossification involving bone deposition within tissue due to severe quadriceps contusion from direct blow or repetitive blows to anterior and lateral thigh • Hip pointer • Contusion to an unprotected iliac crest that can be traumatic in nature to fracture.
Myositis ossificans • Abnormal ossification involving bone deposition with in muscle tissue • Common in quadriceps contusion • Caused by single blow or repeated blows to area • Anterior and Lateral thigh are common sites • Evidence of calcification on a radiograph is visible after 3-4 weeks
Hip Pointer • Contusion to iliac crest • Due to abdominal and trunk muscle attachment any movement is painful • Signs: discoloration, spasm, loss of function • In severe cases crutches will be necessary • Can cause fx. of iliac crest: avulsion of sartorius muscle
Common Injuries • Piriformis Syndrome • Spasms or hypertrophy of the piriformis places pressure on the sciatic nerve, mimicking the signs & symptoms of lumbar nerve root compression or sciatica in the buttock or posterior leg • Resisted abduction of the hip reproduces the pain
Common Injuries • Bursitis • Trochanteric Bursitis • Occurs at the greater trochanter • Iliopsoas Bursitis • Occurs at the lesser trochanter • Ischial Bursitis • Pain usually do to a direct blow or fall on the ischial tuberosity
Common Injuries • Chronic Bursitis • Can lead to snapping hip syndrome • Athletes that ER the hip repetitively. This motion causes the iliotibial tract snaps over the greater trochanter or the snapping in the medial groin • Traumatic hip dislocations • Due to violent twisting actions or car accidents where knees are jammed into the dash board. • Sprains • Occur to Acetabulofemural and Sacroiliac ligs. Surrounding the pelvic region
Common Injuries • Strains • Hamstrings Strain • The most frequently strained muscle • Could become a chronic problem for the athlete • Adductor Strain • Common in sports that require quick changes of direction & explosive propulsion & acceleration • Quadriceps Strains • Common in Sartoris, ilipsoas, and rectus femoris *** The key is early detection ***
Common Injuries • Vascular Disorders • Legg-Calve-Perthes Disease • Avascular necrosis of the proximal femoral epiphysis. • Caused by diminished blood supply to the capital region of the femur
Common Injuries • Vascular Disorders • Thrombophlebitis • An acute inflammation of the vein phlebothrombosis is a clotting in a vein without overt inflammatory signs or symptoms. • Two types • Superficial Thrombphlebitis • Deep Thrombophlebitis
Common Injuries • Hip fractures • Avulsion Fractures • occur during explosive muscular contractions against fixed resistance or during rapid acceleration • Common sites • ASIS, AIIS, Ischial tuberosity, Lessor Trochanter • Femoral Fractures’ • Unusual but very serious injury • Open or closed fracture with significant bleeding at fracture site
Common Injuries • Hip Fractures • Ephiphyseal Fractures • Slipped Capital Femoral Epiphysis • A congenital disorder that develops over time • Usually seem in adolescent boys age 8-15 occurring across the capital femoral epiphysis