Download
1 / 14
140 likes | 158 Views
Six Sigma at Academic Medical Hospital. The following presentation was developed by Jane McCrea, Black Belt of the ED Wait Time Project at Academic Medical Hospital. The presentation follows the DMAIC methodology. Six Sigma--DMAIC.

E N D
Six Sigma at Academic Medical Hospital The following presentation was developed by Jane McCrea, Black Belt of the ED Wait Time Project at Academic Medical Hospital. The presentation follows the DMAIC methodology.
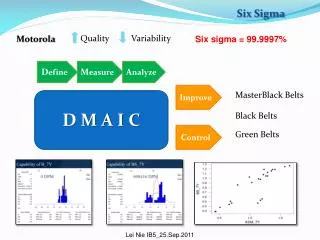
Six Sigma--DMAIC • Define: Define and scope problem. Identify potential benefits and critical to quality (“CTQ”) factors. • Measure: Identify the key internal process that influences CTQ characteristics and measure the defects generated relative to the identified CTQs. Confirm measurement system reliability. Know voice of customer. End result: team can successfully measure the defects generated for a key process affecting the CTQ. • Analyze: Identify root causes of defects. Use statistical data tools to identify key process inputs that affect process outputs. End result: explain variables that are likely to drive process variation the most. • Improve: Determine and confirm optimal solution (statistically re-analysis). Identify the maximum acceptable ranges of key variables. End result: modify the process to stay within the acceptable ranges. • Control: Ensure that modified process now enables the key variables to stay within the maximum acceptable ranges using tools such as metric dashboards and accountability reporting.
Define MD Nurse Tx Room Register Arrival Lobby Triage ED Wait Time Champion Dr. Gerry ElbridgeSponsor Dr. Terry Hamilton Black Belt Jane McCrea Green Belt Dr. James Wilson Foundations Team Nancy Jenkins, Bill Barber, Georgia Williams, Steve Small six sigma The Way We Work Project Description Reduce and consistently maintain patient wait times from triage start to first physician interaction at established thresholds. • EXPECTED BENEFITS • Customer: Critical to Quality (CTQ) • Reduce Wait Time • Internal: Critical to Quality (CTQ) • Improve Patient/Staff Satisfaction • Enhance Patient Outcomes • Increase ED capacity and operational efficiency
Measure What was the Voice of the Customer? • Patient Survey • N = 30; Priority II Patients • Random: all days, all shifts • Patient Survey Results • Wait Time Expectations: • 10-20 minutes: 43% • 20-30 minutes: 23% • Patient Survey Results • Wait Time Satisfaction • Very Satisfied: 37% • Very Dissatisfied: 37%
Baseline Measurements An observational prospective manual time study yielded baseline measurements for the total wait time • Triage Start to • MD Start • Mean: 62.5 min. • Std. Dev: 39.66 • Z-Score: 1.79 • Defect Rate: 38.6% • USL: 37.1 min. 20 60 100 140 180
Measure What did we measure? • Y:# of Minutes, from Triage Start to First Physician Interaction • Specification Limit:37 minutes • Specification Validation:Internal experts & data, External benchmarks • Defect:Wait time > 37 minutes • Unit:One priority II patient visit with one defect opportunity each • Measurement System:Patient Survey, Manual Data Collection, Chart Review, Quality Reports, Registration & Staffing Reports • Impact on Business: • 25 min. Line of Sight Reduction Per Patient Resulting = Capacity Opportunity • Improved Patient Satisfaction, Reduced Complaints, Enhanced Outcomes • Improved Staff Satisfaction & Reduced Turnover • Improved Daily ED Operational Efficiency Key Takeaway: 40% Wait Reduction & Operating Margin Gains
What critical X’s were tested as being root causes of the problem? Environment People Materials Analyze ED patient volume ED patient acuity Influx of squad patients Referral volume Clinics schedules OR volume Hospital patient volume ED tx room limits/facility constraints Staffing levels Experience & skill level Resident specialty Volunteer/greeter utilization Family needs Role clarification Match of skill sets and assignments Variation of practice Availability of supplies Triage process Registration/Chart prep process Charting procedures Communication Availability of diagnostic equipment Availability of trams, pumps, etc. Non-optimization of Tracking system Inadequate IS system for tracking/trending No Physician Prescription Writing system No integrated, on-line charting system Quality of measurement Are we measuring the right things? What do we do with what we measure? Need to do more than “track” Feedback systems to quality auditing Need for Improved flow sheet format Lack of on-line charting system for automated monitoring Utilization of minor emergency unit Ancillary services levels Specialty testing delays ED used as admission unit ED discharge practice Hospital discharge process/timing Consult responsiveness/practices Use of ED for boarding Measure Machines • 23 variables & 18 time stamps • Analyzed via 2nd. wave of data collection • Patient Volume-Related: 10 • Staffing Volume-Related: 5 • Staffing Mix-Related: 5 • Misc: 3 Segmentation/delineation Sequential care vs. parallel processes Methods Improvement implementation/maintenance ownership
Improve What critical X’s were tested as being root causes of the problem? • 23 variables selected & analyzed • through second wave of data collection • Census-Related: 10 • Staffing Related: 5 • Coded: 5 • Miscellaneous: 3 What root causes were confirmed and tested in the pilot? Patient Flow • Direct-to-bed flow & bedside registration • Patient relocation to semi-private space when appropriate • Flow Facilitator Care Team Communication • Modified Zoning • Communication Board • Clinical Protocols Streamlined Order Entry & Results Retrieval Process
Pilot Design Fishbone diagramming, data collection and statistical analysis determined the Critical X’s (contributing factors) as key components for the randomized pilot. • Patient Flow • Direct-to-bed flow; Relocation to semi-private space • Care Team Communication • Zoning; Communication board; Clinical protocols • Streamlined Order Entry & Results Retrieval • Uses central clerk
Improve What were the pilot factors and results? Patient Flow • Direct-to-bed flow & bedside registration • Patient relocation to semi-private space when appropriate • Flow Facilitator Care Team Communication • Modified Zoning • Communication Board • Clinical Protocols Streamlined Order Entry & Results Retrieval Process
PILOT CONCLUSIONS Mood’s Median Test • Pilot lobby wait times were better than the established 15 min. target, the defect rate tumbled, and the C.I. validated statistical significance. • Results for MD wait times were statistically significant in one of two Mood’s median tests. Positive trending was demonstrated in the comparison of Study 2 to the Pilot. • Stakeholders supported department-wide, multi-patient population implementation.
Control What are the building blocks of Control? Guidelines & Assigned Responsibility • New Standard Operating Procedure • Detailed Who, What and When plan Data Review, Reporting & Accountability • Quarterly manual/automated data analysis • Monthly reports and control charts • Use of Corrective Action Log per guidelines • Monthly reports • Scheduled reporting to executive leadership • Quarterly review to owner peers & executives Communication & Recognition • Monthly updates to dept. communication center & newsletter • Monthly updates at staff, faculty & resident meetings • Incorporation of staff recognition for ongoing positive results