Download
1 / 20
270 likes | 781 Views
Drug presentation 1 agonist/antagonist. Barry Barkinsky EMS-I, Paramedic. Receptor sites. Drugs either stimulate or inhibit the cells normal biochemical actions. Receptor sites. Point of attachment for hormones, viruses, chemicals. Agonist / antagonist. Lock and key analogy.

E N D
Drug presentation 1agonist/antagonist Barry Barkinsky EMS-I, Paramedic
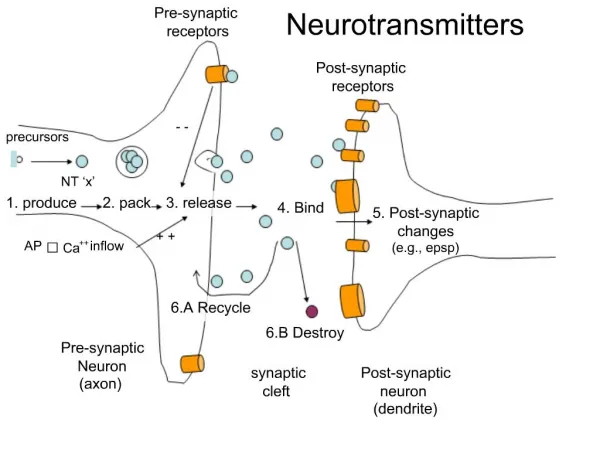
Receptor sites.. • Drugs either stimulate or inhibit the cells normal biochemical actions
Receptor sites • Point of attachment for hormones, viruses, chemicals
Lock and key analogy • Agonist works like a lock and key that works
Agonists • Bind to the receptor site and initiate the expected response • If you put the key in the lock and turn it the lock will open • Side effect
Morphine sulfateclass: opioid agonist • Prototype drug: • Causes analgesia, euphoria, sedation and miosis. • Decreases preload and afterload. • May cause respiratory depression and hypotension.
Morphine…mechanism • Opiate agonist • Cause the desired effect of pain relief • Also opens doors to respiratory depression and hypotension • Has successfully opened doors to: • Pain relief / High • Respiratory depression • Hypotension via vasodilation
Morphine sulfate • Indications • Moderate to severe pain • Cardiac pain indicative of MI • Acute pulmonary edema • Precautions: • Hypersensitivity, undiagnosed head or abdomen injury, bronchial asthma, COPD, severe respiratory depression, pulmonary edema due to chemical agent
Fentanyl (sublimaze) • potency many times that of morphine. • Schedule II drug • Also seen as duragesic or actiq • High potential for respiratory depression • Anesthetic and analgesic – dose dependant
Fentanyl (sublimaze)synthetic narcotic analgesic • Indications: Induce sedation for endotracheal intubation. • Contraindications: MAO inhibitors within 14 days, myasthenia gravis. • Precautions: Increased intracranial pressure, elderly, debilitated, COPD, respiratory problems, hepatic and • renal insufficiency. • Dosage/Route: 25 to 100 mcg slowly IV (2 to 3 min). Ped: 2 mcg/kg slow IV/IM.
Stadol • Name/Class: BUTORPHANOL (Stadol)/Synthetic Narcotic Analgesic • Description: Butorphanol is a centrally acting synthetic narcotic analgesic about 5 times more potent than morphine. A schedule IV narcotic. • Indications: Moderate to severe pain. • Contraindications: Hypersensitivity, head injury, or undiagnosed abdominal pain. • Precautions: May cause withdrawal in narcotic-dependent patients • Dosage/Route: 1 mg IV or 3 to 4 mg IM/3 to 4 hours.
Noncompetitive antagonism • The antagonism is insurmountable • Example:You can’t effectively push CO off of hemoglobin once its got the site
Competitive antagonism • Considered surmountable • Enough of an agonist can overcome the antagonism
Competitive Antagonists • Bind to the site but do not cause the receptor to initiate the expected response • The key fits in the lock but will not turn and cannot open the lock – however the lock is now blocked
Opioid antagonists • Reverse some of the effects of opioid drugs • Typically desired for respiratory depression effect • Shorter half life than most opioid drugs
Reversal • Naloxone: opiate antagonist • Binds to opiate receptor – fits in lock but doesn’t turn it – blocks it • Doesn’t elicit the desired response: • No pain relief / No high– door blocked • No respiratory depression – door blocked • Can’t bind to the receptor causing vasodilation morphine has bound to – so hypotension is not reversed – door NOT blocked • Morphine----->>>> • Pain relief / High • Respiratory depression • Hypotension
Naloxone (narcan) • Prototype opioid antagonist drug • Repeat doses may be needed to combat shorter half life • Competitively binds with opioid receptors without causing the effects of opioid binding. • Primary binding is at respiratory centers – it will not reverse hypotension
narcan • Indication: • Natural of synthetic narcotic overdose • Coma of unknown origin • Precaution: shorter half life than most of the drugs it antagonizes • Dosage/Route: 0.4 to 2.0 mg IV/IM, 2 to 2.5X ET up to 10 mg, 2 mg MAD