Download
1 / 34
340 likes | 356 Views
This report provides an overview of Lyme disease, its prevalence in Rhode Island, the response of the medical community, analysis of clinical guidelines, insurance coverage, and current long-term goals. It includes data on Lyme disease cases, physician survey results, treatment best practices, and gaps in insurance coverage.

E N D
Report on Lyme Disease Response to PL 2015, R431 and PL 2014, R087 March 3, 2016 Nicole Alexander-Scott, MD, MPH
Presentation Overview • Lyme disease overview • Lyme disease in Rhode Island • Medical community and Lyme disease • Analysis of Lyme disease clinical guidelines • Insurance coverage for Lyme disease • Current and long-term goals
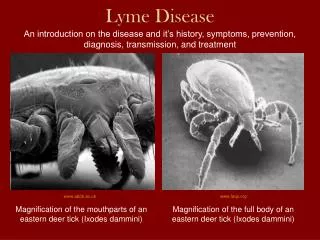
Lyme Disease Overview • Caused by bacterium Borreliaburgdorferi • Spread through bite of infected black-legged (deer) tick • In most cases, a tick must be attached for 36 to 48 hours or more for Lyme disease bacterium transmission
Lyme Disease Symptoms • Typical initial symptoms • Bull’s-eye rash (erythema migrans) in 60%-80% of patients within 7 to 30 days of tick bite • Non-specific symptoms: fever, tiredness, headache, joint pain, muscle pain • Late manifestations (weeks – months after bite) • Arthritis (particularly in the knee joint) • Neurologic problems (Bell’s Palsy) • Cardiac issues • Meningitis • Chronic Lyme/Post Treatment Lyme Disease Syndrome
Topic 1Analysis of Current Levels of Lyme Disease in Rhode Island
Lyme Disease in Rhode Island2008-2015 Passive Surveillance Active Surveillance *2015 data are provisional
Lyme Disease by Age, 2014 • Adults ages 50-59 had the highest rate • People ages 60-69, 10-19 had the second highest rate
Lyme Disease by Sex • Males had higher counts and rates of Lyme disease than females • Consistent with 10-year trend of national data
Lyme Disease by Month • Lyme disease peaks in the summer when people spend more time outside • Nationally, Lyme disease peaks in the summer too • 2014: 59% of Lyme disease cases were June - August
Topic 2Response of the Medical Community in Treating Lyme Disease
Physician Survey • November 2015 – January 2016 • Surveyed primary care physicians • Questions about knowledge, attitudes, and practices (diagnostic and treatment) regarding Lyme disease • 211 respondents
Physician Survey Respondents’ knowledge • 19% do not know Lyme disease is endemic (widespread) in Rhode Island • 19% do not know how long a tick must be attached in order to transmit Lyme disease • 50% do not know serologic tests for Lyme disease cannot be used to distinguish between active and past infection • 56% do not know all Lyme disease cases, by law, are reportable to RIDOH
Physician Survey Respondents’ diagnosing practices • 42% reported offering no patient education about Lyme disease in the office • Test-ordering practices are quite variable • Antibiotic prescribing is quite variable • 32% reported they would prescribe antibiotics to patient who requests it for Lyme disease, even if patient is asymptomatic and has no history of a tick bite
Topic 3Analysis of Best Practices in the Treatment of Lyme Disease
Long-Term Antibiotic Therapy Research IDSA/CDC ILADS Observational case series Confirmed diagnosis of Lyme not required for all Most frequent antibiotics used were macrolides and tetracyclines in conjunction with anti-inflammatories Length of therapy: 3 - 6 months No difference in outcomes between seronegative vs. seropositive patients Outcome was patient-reported improvement in symptoms (subjective) • 4 randomized, placebo controlled clinical trials • Outcomes measured using validated scoring scales • No sustained difference in outcome measures between placebo and treatment groups at end of study • Higher rate of adverse events in treatment group vs. placebo group (26% vs. 7%) • Multiple hospitalizations in all studies in treatment group arm for adverse events
Topic 4Gaps in Insurance that Affect Access to Treatment of Lyme Disease
Insurance Coverage forLyme Disease Treatment • Chapter 5-37.5: requires health plans to provide for Lyme disease treatment • “No physician is subject to disciplinary action solely for prescribing, administering, or dispensing long-term antibiotic therapy for a patient clinically diagnosed with Lyme disease, if this diagnosis and treatment plan have been documented in the patient’s medical record.” • Lyme disease treatments, like other treatments, must be “medically necessary” and “appropriate”
Insurance Coverage forLyme Disease Treatment Lyme treatments are generally covered by insurance. Like other diseases/conditions, there are several reasons why treatments might be not covered or partially covered: • Not medically necessary/appropriate • Coding errors • Over-the-counter products • Laboratory/provider is out-of-network • Provider only accepts cash payments • Patient’s employer is self-insured • Deductibles/copays • Other conditions
Insurance Coverage forLyme Disease Treatment Patient options if coverage denied • The Rhode Island Department of Health (RIDOH) and the Rhode Island Office of the Health Insurance Commissioner (OHIC) oversee denials and check to ensure that: • Patient due process rights are honored • Decisions made are reasonable • Criteria used to make decisions is sound • Patient can also contact Rhode Island’s toll-free Health Insurance Consumer Support Line (RI Reach): 855-747-3224.
Topic 5Current and Long-Term Goals and Strategies to Address the High Incidence of Disease in the State
Short and Long-Term Goals • Current Activities • Active surveillance • Public education • Provider education • Future Activities • Continue support for public and provider education • Coordinate with DEM, URI • Coordinate with New England states • Stay current on Lyme research
Current Activities • Active disease surveillance • Provider outreach and education • Public awareness and education • Strengthening partnerships
Provider Education • Healthcare provider e-newsletters • Individualized education with providers • Comprehensive website for physicians
Public Education • One Bite preventioncampaign • Media interviews • Press releases • Website • Social media • Tick tool kit (summer camps)
Public Advertising • Posters on buses, Block Island Ferry • Paw Sox (radio show, game-day interviews, fan mailings, jumbo-tron) • Print ads in Rhode Island Summer Guides • Tick safety signs posted at state parks
Strengthening Partnerships • Education materials distributed at Great Outdoor Pursuit events • Train-the-trainer workshops for DEM, DOT for tick safety - Educational materials - Signage - Tick-identification magnets - Permethrin (tick repellant) • Paw Sox
Long-Term Goals • Promote continued research on diagnosis and treatment of Lyme disease • Coordinate with New England states • Enhance provider outreach and education, emphasizing clinical research updates and innovations in the diagnosis and treatment of tick-borne illness • Maintain active disease surveillance
Long-Term Goals • Continue public awareness campaigns, as federal funds allow, and seek partners for additional sustainable, low-cost public awareness opportunities • Increase outreach to those communities most impacted by Lyme • Provide targeted trainings and workshops, based on funding
Conclusion • There is a need to more accurately reflect the burden of disease with increased testing, diagnosis, and reporting • We must continue and enhance education for providers and the public • There are still unanswered questions--we need reliable data and research
CDC case definitions Suspected • A case of EM where there is no known exposure (as defined) and no laboratory evidence of infection (as defined), OR • A case with laboratory evidence of infection but no clinical information available (laboratory report). Probable • Any other case of physician-diagnosed Lyme disease that has laboratory evidence of infection (as defined). Confirmed • A case of EM with a known exposure (as defined), OR • A case of EM with laboratory evidence of infection (as defined) and without a known exposure OR • A case with at least one late manifestation that has laboratory evidence of infection.