VENTILATOR THE BASIC- COURSE
VENTILATOR THE BASIC- COURSE. HISTORY OF VENTILATOR. Early History of Ancient times . Old testament there is a mention of Prophet Elisha Inducing pressure breathing from his mouth into the mouth of a child who was dying–(Kings 4:34-35). . Hippocrates (460-375 BC) wrote


VENTILATOR THE BASIC- COURSE
E N D
Presentation Transcript
VENTILATOR THE BASIC- COURSE
HISTORY OF VENTILATOR
Early History of Ancient times Old testament there is a mention of Prophet Elisha Inducing pressure breathing from his mouth into the mouth of a child who was dying–(Kings 4:34-35). Hippocrates (460-375 BC) wrote the first description of endotracheal intubation his book –‘Treatise on Air’ “One should introduce a cannula into the trachea along the jaw bone so that air can be drawn into the lungs”.
Negative Pressure Ventilators Two successful designs became popular; In one - the body of the patient was enclosed in an iron box or cylinder and the patient’s head protruded out of the end. The second - design was a box or shell that fitted over the thoracic area only (chest cuirass).
IRON LUNG- DRINKER LUNG (Philip Drinkerand Louis Agassiz Shaw)mid-1900s The first iron lungwas used on October 12, 1928at Children's Hospital,Boston, -used in a child unconscious from respiratory failure; -her dramatic recovery, within seconds popularize the "Drinker Respirator."
In 1949, John Haven Emerson Developed a mechanical assister for anesthesiaat Harvard University.
Iron lung ward filled with Polio patients, Rancho Los Amigos Hospital, ca. 1953
During the 1950's Mechanical ventilators used increasingly in Anesthesia and intensive care. -To treatpoliopatients and -The increasing use ofmuscle relaxants during anesthesia
THE COURSE DEALS WITH • INTRODUCTION • INDICATION FOR MECHANICAL VENTILATION • MECHANICAL VENTILATOR- WHAT IT IS ? • MECHANICAL VENTILATORS- CLASSIFICATION • VENTILATOR MODES • HOW TO INITIATE MECHANICAL VENTILATION? • VENTILATOR SETTINGS • NURSING CARE • SEDATION AND NEUROMUSCULAR BLOCKADE • ASSESMENT CRITERIA • WEANING AND EXTUBATION • FAILURE TO WEAN • METHODS OF WEANING • POST EXTUBATION CARE
P0ST-TEST EVALUATION HANDS ON VENTILATOR HANDS ON INTUBATING MANNIQUINE
WHAT A MOST IMPORTANT THING A DOCTOR SHOULD KNOW AFTER THIS COURSE ? MONITORING THE PROGRESS
WHAT A MOST IMPORTANT THING A ICU STAFF SHOULD KNOW AFTER THIS COURSE ? ALARMS AND CARE OF THE PATIENT
Mechanical ventilation is used when a patient is unable to breathe adequately on his or her own. • The ventilator can either completely take over respiratory function, or it can be used to support the patient’s own respiratory efforts
MECHANISM OF RESPIRATION A mechanism for telling the body that it is time to breath: This involves CO2 sensors in the brainstem, which signal diaphragmatic movement via the cervical nerves. The phrenic nerves The diaphragm contracts – it increases the volume of the thorax, by moving down into the abdomen, making the intra-pleural and intra-alveolar pressure more negative, creating a pressure gradient between the atmospheric and the alveoli, and allowing air to pass down through a series of narrowing bronchi into the alveoli. The alveoli and the pulmonary capillary network, Derived from the main pulmonary arteries, oxygen and carbon dioxide diffuse across the concentration gradient out of and into the alveoli respectively. The diffusion of CO2 is more effective due to it’s higher solubility.
Indications for mechanical ventilation: Ventilation Failure Oxygenation Failure
Failure to Ventilate Characterized by reduced alveolar ventilation which manifests as an increase in the PaCO2 > 50 mmHg
Indications for mechanical ventilation: • Is itfailure to ventilate(is the PCO2 > 50mmHg), orfailure to oxygenate(is the PO2 <50mmHg)? • Remember that a low O2 is much more significant than a high PCO2, • If it isventilatory failure, where is the injury – in the brain (the medulla), - in the spinal cord, - in the peripheral nerves, - at the neuromuscular junction, - in the muscle itself or in the chest cage? • If the problem isoxygenation failure, where is the injury: - Is it in the blood supply, - at the alveolar-capillary interface or - in the upper, middle or lower airways?
Neurological Problems ( Ventilatory failure ) • Central: Loss of ventilatory drive due to sedation, narcosis, stroke or brain injury. • Spinal: Spinal cord injury, cervical – loss of diaphragmatic function, thoracic – loss of intercostals. • Peripheral:Nerve injury (e.g. phrenic nerve in surgery), Guillain-Barre syndrome (demyelination), poliomyelitis, motor neurone disease. • Muscular Problems – myasthenia gravis, steroid induced myopathy, protein malnutrition. • Anatomical Problems Chest Wall– rib fractures or flail chest, obesity, abdominal hypertension, restrictive dressings Pleura– pleural effusions, pneumothorax, hemothorax. Airways – airway obstruction (in lumen, in wall, outside wall), laryngeal edema, inhalation of a foreign object, bronchospasm
Failure to Oxygenate Diffusion abnormality– Thickening of the alveoli (fibrosis) Increased extracellular fluid – pulmonary edema. This obstructs gas exchange. • Ventilation/Perfusion Mismatch :Dead Space Ventilation • (or high V/Q)– • Alveoli are ventilated but not perfused Eg; pulmonary embolus • Dead space may be anatomical - the conducting airways(150ml) • physiological, for example in hemorrhage or hypotension Shunt (or low V/Q)–where alveoli are perfused but not ventilated occurs in airway collapse, pneumonia, pulmonary hemorrhage (contusion), ARDS/ALI. Inability to extract O2 at cellular level–sepsis, cyanide or carbon monoxide poisoning
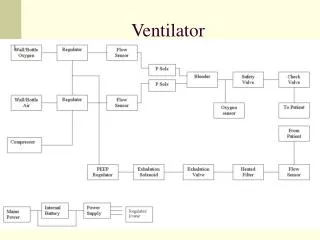
Mechanical Ventilator What is it?
Mechanical Ventilator What is it? Amechanical ventilatoris a machine that generates a controlled flow of gas into a patient’s airways Two kinds of ventilators: Negative pressure and Positive pressure. Negative Pressure : -iron lung, the Drinker respirator, and the chest shell -advantage these ventilators didn’t require insertion of an artificial airway, -disadvantage they were noisy and made nursing care difficult. Positive Pressure : -The Emerson Company in Boston developed the positive pressure ventilator, which was first used at Massachusetts General Hospital.
Positive pressure ventilators • Require an artificial airway (endotracheal or tracheostomy tube), • and use positive pressure to force oxygen into a patient’s lungs • Inspiration can be triggered either by the patient or the machine. • Four types of positive pressure ventilators: • volume cycled • pressure cycled -deliver a preset tidal volume -ideal for patients with bronchospasm since the same tidal volume is delivered regardless of the amount of airway resistance -deliver gases at preset pressure -decreased risk of lung damage from high inspiratory pressures -disadvantage is that the patient may not receive the complete tidal volume if he or she has poor lung compliance and increased airway resistance
flow cycled • time cycled -deliver a breath until a preset flow rate These aren’t used -deliver a breath over a preset time period expiration is passive . gas flows along a pressure gradient between the upper airway and the alveoli Flow is either volume targeted and pressure variable, or pressure limited and volume variable. The pattern of flow may be either sinusoidal (which is normal), decelerating or constant. Flow is controlled by an array of sensors and microprocessors.
Mechanical Ventilators Classification
Mechanical Ventilators Classification 1) Control Either Volume Controlled(volume limited, volume targeted) and Pressure VariableorPressure Controlled(pressure limited, pressure targeted) and Volume VariableorDual Controlled(volume targeted (guaranteed) pressure limited) 2) Cycling: Time cycled- such in in pressure controlled ventilation Flow cycled- such as in pressure support Volume cycled- the ventilator cycles to expiration once a set tidal volume has been delivered: this occurs in volume controlled ventilation -If an inspiratory pause is added, then the breath isboth volume and time cycled (contd)
3) Triggering: • what causes the ventilator to cycle to inspiration? • Ventilators may be • time triggered, • pressure triggered or flow triggered. • Time:the ventilator cycles at a set frequency as determined by the • controlled rate. • Pressure:the ventilator senses the patient's inspiratory effort • by way of a decrease in the baseline pressure. • Flow:modern ventilators deliver a constant flow around the circuit • throughout the respiratory cycle (flow-by). A deflection in this • flow by patient inspiration, is monitored by the ventilator and • it delivers a breath. • This mechanism requires less work by the patient than pressure triggering. • (Contd)
4) Breaths are either: what causes the ventilator to cycle from inspiration? • Mandatory (controlled) -which is determined by the respiratory rate. • Assisted - (as in assist control, synchronized intermittent mandatory ventilation, pressure support) • Spontaneous- (no additional assistance in inspiration, as in CPAP) • 5) Flow pattern: • constant, accelerating, decelerating or sinusoidal • Sinusoidal =this is the flow pattern seen in spontaneous breathing and CPAP • Decelerating =the flow pattern seen in pressure targeted ventilation: • inspiration slows down as alveolar pressure increases • (there is a high initial flow). • (Contd)
Constant -flow continues at a constant rate until the set tidal volume is delivered • Accelerating-flow increases progressively as the breath is delivered. This should not be used in clinical practice. Flow Pattern
KEY-POINTS 1. Theresting point of outward chest spring and inward lung collapse is the Functional Residual Capacity (FRC): this is a reservoir for gas exchange .The FRC is the lung’s physiologic reserve, it is a reservoir. 2. Loss of chest wall or lung compliance causes reduced FRC. 3. Exhalation below FRC is active causing dynamic airway collapse, trapping air in the alveoli (auto PEEP) 4. At residual volume it is not possible to empty alveoli of air further, due to dynamic airway collapse (airway closure) 5. The closing volume (CV) is the point at which dynamic compression of the airways begins. 6. Such airway closure occurs normally within FRC, and it is known as the closing volume (CV). With age and disease the CV moves into the tidal breathing range. 7. The CV increases with age, smoking, lung disease, and body position (supine > erect). 8. Airway collapse increases the work of breathing and leads to ventilation-perfusion mismatch 9. In mechanically ventilated patients airway collapse is prevented by applying positive pressure to the airway throughout the respiratory cycle – CPAP/PEEP 10. PEEP/CPAP works by increasing FRC, maintaining alveolar recruitment facilitating gas exchange (and removal of CO2 and replenishment of O2), and reducing the workload of breathing. 11. The patient requires sufficient PEEP to prevent alveolar de-recruitment, but not so much PEEP that alveolar over-distension, dead space ventilation and hypotension occurs. 12. The ideal level of PEEP is that which prevents de-recruitment of the majority of alveoli, while causing minimal over-distension. 13. Recruitment maneuvers are used to re-inflate collapsed alveoli, a sustained pressure above the tidal ventilation range is applied, and PEEP is used to prevent de-recruitment. 14. Auto-PEEP is gas trapped in alveoli at end expiration, due to inadequate time for expiration, bronchoconstriction or mucus plugging. It increased the work of breathing. 15. The increased work of breathing associated with auto-PEEP can be offloaded by applying CPAP to the trachea/mouth, and splinting open the connecting airways. The objective is to set the CPAP level above the auto-PEEP level.
Ventilator Waveforms Airway pressure screen Step 1: - determine the CPAP level – this is the baseline position from which there is a downward deflection on, at least, beginning of inspiration, and to which the airway pressure returns at the end of expiration. Step 2: is the patient triggering? -There will be a negative deflection into the CPAP line just before inspiration
Step 3: what is the shape of the pressure wave? -If the curve has a flat top, then the breath is pressure limited, if it has a triangular or shark’s fin top, then it is not pressure limited and is a volume breath. Flow screen: Step 4: what is the flow pattern? – If it is constant flow (square shaped) this must be volume controlled, if decelerating, it can be any mode.
Is the patient gas trapping? – -expiratory flow does not return to baseline before inspiration commences (i.e. gas is trapped in the airways at end-expiration). Step 4:the patient is triggering – is this a pressure supported or SIMV or VAC breath? -This is easy, the pressure supported breath looks completely differently than the volume control or synchronized breath: the PS breath has a decelerating flow pattern, and has a flat topped airway pressure wave. The synchronized breath has a triangular shaped pressure wave. Airway pressure Flow pattern
Step 5: the patient is triggering – is this pressure support or pressure control? -The fundamental difference between pressure support and pressure control is the length of the breath – in PC, the ventilator determined this (the inspired time) and all breaths have an equal “i” time. In PS, the patient determined the duration of inspiration, and this varies from breath to breath.
Step 6: is the patient synchronizing with the ventilator? -Each time the ventilator is triggered a breath should be delivered. If the number of triggering episodes is greater than the number of breaths, the patient is asynchronous with the ventilator. Further, if the peak flow rate of the ventilator is inadequate, then the inspiratory flow will be "scooped" inwards, and the patient appears to be fighting the ventilator. Both of these problems are illustrated below
Ventilator Modes • Control Ventilation (CV) • Assist-Control Ventilation (A/C) • Synchronous Intermittent Mandatory Ventilation (SIMV) • Pressure Support Ventilation (PSV) • Positive End Expiratory Pressure (PEEP) • Constant Positive Airway Pressure (CPAP) • Independent Lung Ventilation (ILV) • High Frequency Ventilation (HFV) • Inverse Ratio Ventilation (IRV) • Advanced Pressure Control Modes • -Inverse Ratio Ventilation (IRV) and -Airway Pressure Release Ventilation (ARPV), • -Bilevel and Proportional Assist Ventilation?
1)Control Ventilation (CV) -CV delivers the preset volume or pressure regardless of the patient’s own inspiratory efforts. -This mode is used for patients who are unable to initiate a breath. -If it is used with spontaneously breathing patients, they must be sedated and/or pharmacologically paralyzed so they don’t breathe out of synchrony with the ventilator.
2)Assist-Control Ventilation (A/C) -A/C delivers the preset volume or pressure in response to the patient’s own inspiratory effort but will initiate the breath if the patient does not do so within the set amount of time. -This means that any inspiratory attempt by the patient triggers a ventilator breath. -The patient may need to be sedated to limit the number of spontaneous breaths since hyperventilation can occur. -This mode is used for patients who can inititate a breath but who have weakened respiratory muscles.
3) Synchronous Intermittent Mandatory Ventilation (SIMV) -SIMV was developed as a result of the problem of high respiratory rates associated with A/C. -SIMV delivers the preset volume or pressure and rate while allowing the patient to breathe spontaneously in between ventilator breaths. -Each ventilator breath is delivered in synchrony with the patient’s breaths, yet the patient is allowed to completely control the spontaneous breaths. -SIMV is used as a primary mode of ventilation, as well as a weaning mode. -The disadvantage of this mode is that it may increase the work of breathing and respiratory muscle fatigue.
4) Pressure Support Ventilation (PSV) -PSV is preset pressure that augments the patient’s spontaneous inspiratory effort and decreases the work of breathing. -The patient completely controls the respiratory rate and tidal volume. -PSV is used for patients with a stable respiratory status and is often used with SIMV to overcome the resistance of breathing through ventilator circuits and tubing.
5) Positive End Expiratory Pressure (PEEP): -PEEP is positive pressure that is applied by the ventilator at the end of expiration. -Used as an adjunct to CV, A/C, and SIMV to improve oxygenation by collapsed alveoli at the end of expiration. -Complications decreased cardiac output, pneumothorax, and increased intracranial pressure.
6) Constant Positive Airway Pressure (CPAP) -CPAP is similar to PEEP except that it works only for patients who are breathing spontaneously. -The effect of both is comparable to inflating a balloon and not letting it completely deflate before inflating it again. The second inflation is easier to perform because resistance is decreased. -CPAP can also be administered using a mask.
7) Independent Lung Ventilation (ILV) -This method is used to ventilate each lung separately in patients with unilateral lung disease or with a different disease process in each lung. -It requires a double-lumen endotracheal tube and two ventilators. -Sedation and pharmacological paralysis are used to facilitate optimal ventilation and increased comfort for the patient. 8) High Frequency Ventilation (HFV) -HFV delivers a small amount of gas at a rapid rate (as much as 60-100 breaths per minute.) -This is used when conventional mechanical ventilation would compromise hemodynamic stability, during short-term procedures, or for patients who are at high risk for pneumothorax. -Sedation and pharmacological paralysis are required.
9) Inverse Ratio Ventilation (IRV) -The normal inspiratory:expiratory ratio is 1:2 but this is reversed during IRV to 2:1 or greater (the maximum is 4:1). -This mode is used for patients who are still hypoxic even with the use of PEEP. -The longer inspiratory time increases the amount of air in the lungs at the end of expiration (the functional residual capacity) and improves oxygenation by reexpanding collapsed alveoli. -The shorter expiratory time prevents the alveoli from collapsing again. -Sedation and pharmacological paralysis are required since it’s very uncomfortable for the patient.
MODE FUNCTION CLINICAL USE Control Ventilation (CV)Delivers preset volume or pressure Usually used for patients who are apneic regardless of patient’s own inspiratory efforts Assist-Control Ventilation (A/C)Delivers breath in response to Usually used for spontaneously patient effort and if patient fails to breathing patients with weakened do so within preset amount of timerespiratory muscles Synchronous Intermittent MandatoryVentilator breaths are synchronized Usually used to wean patients from mechanical ventilation with patient’s respiratory effort Ventilation (SIMV) Pressure Support Ventilation (PSV)Preset pressure that augments the Often used with SIMV during weaning patient’s inspiratory effort and decreases the work of breathing Positive End Expiratory Pressure (PEEP)Positive pressure applied at the end Used with CV, A/C, and SIMV to Improve oxygenation by opening collapsed alveoli of expiration Constant Positive Airway PressureSimilar to PEEP but used only with Maintains constant positive pressure in airways so resistance is decreased spontaneously breathing patients (CPAP)