Download
1 / 31
330 likes | 951 Views
PCI v CABG. Dr Rod Stables The Cardiothoracic Centre Liverpool UK. CABG is Alive and Well in Liverpool. CABG is Alive and Well in Liverpool. Liverpool Family Life. Liverpool Family Life. Presentation Outline. Undisputed current facts PCI improves access to revascularisation

E N D
PCI v CABG Dr Rod Stables The Cardiothoracic Centre Liverpool UK
Presentation Outline • Undisputed current facts • PCI improves access to revascularisation • Availability
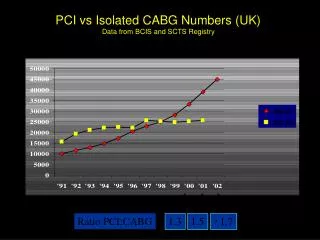
Access to Revascularisation - Availability • Existing immediate capacity • Dominant method for revascularisation • UK PCI growth rate - 16% per annum • UK CABG growth rate - static or negative • Revascularisation event ratio trend > 2 : 1 • Immediate ability to grow capacity favours PCI • NSF targets - and beyond • New indications
Presentation Outline • Undisputed current facts • PCI improves access to revascularisation • Availability • Patients with co-morbidity • Patients with acute presentations • Acute coronary syndromes • Primary PCI for ST MI • Cardiogenic shock
Improved Cardiac Provision Favours PCI • Better primary prevention • Earlier investigation and treatment of CAD • Aggressive early approach to occlusion • Primary PCI for AMI • Early PCI for non-ST elevation ACS • Reduced incidence of • Advanced ‘surgical’ disease’
Presentation Outline • Undisputed current facts • PCI improves access to revascularisation • PCI is cost saving
SoS Trial - Total Costs at 1 Year Cost= £2,609 (95% CI: £1,769 to £3,314) £10,000 £9,000 £1,518 £8,000 Costs £7,000 Follow-up £6,000 £2,412 £5,000 Initial hosp £4,000 £3,000 £2,000 £3,884 £7,321 £1,000 £0 PCI CABG
Presentation Outline • Undisputed current facts • PCI improves access to revascularisation • PCI is cost saving • PCI is popular with patients
PCI - Appeal to Patients • Experience from consent attempts in RCTs • Shorter hospitalstay
SoS Trial: Length of Stay - Index Procedure Median 3 days Median 10 days
PCI - Appeal to Patients • Experience from consent attempts in RCTs • Shorter hospital stay • Reduced immediate procedural morbidity • Avoids GA, scars etc • Rapid rehabilitation • CABG option remains (short or long term)
Presentation Outline • Undisputed current facts • PCI improves access to revascularisation • PCI is cost saving • PCI is popular with patients • PCI is improving at a rapid pace
PCI Evolution • Rate of new product registration • Techniques and application • Adjunctive medication schedules • Imaging equipment • Devices / equipment • Stents and drug eluting stents • Improving clinical results
Presentation Outline • Undisputed current facts • Historic trials favour CABG • Reduced repeat revascularisation
SoS Trial: Repeat Revascularisation Hazard ratio 3.90 (2.58 to 5.91)
SoS Trial: Death or Non-Fatal Q Wave MI Hazard ratio 0.95 (0.63 to 1.43)
Presentation Outline • Undisputed current facts • Historic trials favour CABG • Reduced repeat revascularisation • Emerging clinical data - favours PCI
PCI v CABG: The Current Picture • Non - MACCE adverse events • SoS data • Hospitalisation events after index revasc • Non - MACCE : Never reported • CABG 351 (0.7 per patient) • PCI 156 (0.3 per patient) • MACCE: PCI - superior safety and efficacy
Latest Trials From TCT 2004 • ARTS 2 • Registry n = 607 MV revasc by DES • More diabetes than ARTS 1 (26% v 18%) • More 3 VD (54% v 28%) • More stents (3.7 [73mm] v 2.8 [48mm]) • 6 month freedom from MACCE • ARTS 2 - 93.6 % • ARTS 1: PCI - 84.7% CABG - 94.5%
‘Armies can be resisted but not an idea whose time has come.’ Victor Hugo