Download
1 / 21
310 likes | 1.31k Views
CARPAL TUNNEL SYNDROME Nerve Conduction Study. www.teleemg.com. Katie Doney – kdoney@med.usyd.edu.au. Muscle. CNS. Motor Neuron. Ventral Horn. Motor Pathways. Motor Pathways Possible places of dysfunction. CNS EEG Electroencephalography PET Positron Emission Tomography

E N D
CARPAL TUNNEL SYNDROMENerve Conduction Study www.teleemg.com Katie Doney – kdoney@med.usyd.edu.au
Muscle CNS Motor Neuron Ventral Horn Motor Pathways
Motor Pathways Possible places of dysfunction • CNS • EEGElectroencephalography • PETPositron Emission Tomography • fMRIFunctional Magnetic Resonance Imaging
Motor Pathways Possible places of dysfunction 2. Muscle Needle EMGElectromyography • CNS • EEGElectroencephalography • PETPositron Emission Tomography • fMRIFunctional Magnetic Resonance Imaging
Motor Pathways Possible places of dysfunction 2. Muscle Needle EMGElectromyography • CNS • EEGElectroencephalography • PETPositron Emission Tomography • fMRIFunctional Magnetic Resonance Imaging 3. Peripheral Nerve Nerve conduction study
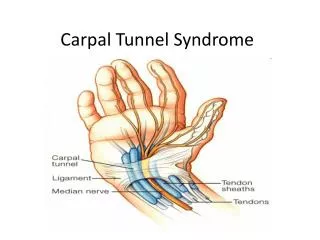
Peripheral Nerve • Made up of: • Sensory nerves • Motor nerves • Myelin • Glial cells MEDIAN ULNAR
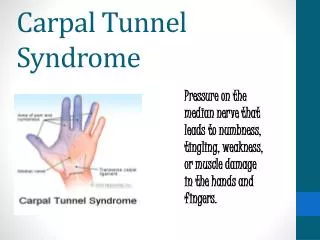
Decreased blood supply Demyelination Axonal degeneration Median Nerve Pathologyin Carpal Tunnel Syndrome • Compression of the median nerve results in • These manifest as: - Numbness - Pain - Parasthesiae - Weakness - Problems with fine manipulative skills
Least sensitive Most sensitive Nerve Conduction Study • Stimulate nerve and record outcome. • 2 main types 1. Motor (record compound muscle action potential) 2. Sensory (record compound sensory action potential) -Orthodromic (stimulate at finger, record on elbow/wrist) -Antidromic (stimulate at elbow/wrist, record on finger) -Radial-median (stimulate at wrist, record on thumb) -Palmar (stimulate at palm, record on elbow/wrist)
Response amplitude Time Changes to CMAP in Carpal Tunnel Syndrome • Latency: Normal < 4.9 ms • Amplitude: Normal ≥ 5 mV • Shape: Normal curve Pathology: - demyelination - axonal degeneration
Nerve Conduction Study • Measures Latency and Amplitude • Latency is the time between the artefact and the initiation of the compound action potential • The artefact occurs when you press the button to stimulate the electrode • Latency increases pathologically due to: • Axonal degeneration • Demyelination • Latency increases non-pathologically due to: • Length of axon
Nerve Conduction Study • Measures Latency and Amplitude • The amplitude of the curve shows the strength of the compound action potential • The area under the curve decreases pathologically due to: • Number of axons involved • Diameter of nerve • The area under the curve decreases non-pathologically due to: • Strength of initial stimulus
Nerve Conduction Study • Motor Nerve Conduction Study Setup: • Stimulating electrode to set up action potentials in median nerve from wrist or elbow • Recording electrode on abductor pollicus brevis to record compound muscle action potential • Techniques to increase effectiveness of stimulation • Earth
r sw 1 r se 2 Conduction Velocity • Importance: Eliminating wrong localisation of problem • Method: Latency wrist Latency elbow
Distance = Lelbow – Lwrist Distance Conduction Velocity Distance • Calculations: Velocity = • Method: Time r sw 1 Latency wrist r se 2 Latency elbow
Conduction Velocity • Normal value > 50 m/s • Other sources of error – stimulus position - estimation of nerve course - latency measurement
Latency CV Age 20 80 Age Problems with comparing features to normal values • Features change with • Temperature • Age • Solution: Repeat measurements on ulnar nerve as a control. This also gives additional evidence to rule out generalised neuropathy.
MEDIAN SENSORY (ANTIDROMIC) ULNAR SENSORY (ANTIDROMIC) - Latency < 3.6 ms - Latency < 3.1 ms - Velocity > 50 m/s - Velocity > 54 m/s - Amplitude > 15 mV - Amplitude > 10 mV Compound Antidromic Sensory Action Potential Setup: - stimulate at wrist/elbow and record at finger - gain set higher - signal very small so average random noise • Normal values:
An example: Right Antidromic Ulnar Normal: -Lat < 3.1 ms -Amp > 10 uV …. Ulnar OK – not generalised neuropathy
An example: Right Antidromic Median Normal: -Lat <3.6 ms -Amp >15 uV -CV >50 m/s …. In median nerve, evidence of demyelination and axonal degeneration between wrist and finger, but not between wrist and elbow. Suggestive of carpal tunnel syndrome.
An example: Right Thenar Median Normal: - Lat < 4.9 ms - Amp ≥ 5 mV - CV > 50 m/s …. Motor portion of median is OK. Mild to moderate carpal tunnel syndrome.
Take home message! • In carpal tunnel syndrome there will be a longer latency between the wrist and the finger/thenar eminence but NOT between the elbow and the wrist • The ulnar nerve will not be effected in carpal tunnel syndrome because it does not pass through the carpal tunnel