Objective
Does Operative Technique of Performing Distal Anastomosis in Acute type A Dissection Affect Early And Late Clinical Outcomes?.

Objective
E N D
Presentation Transcript
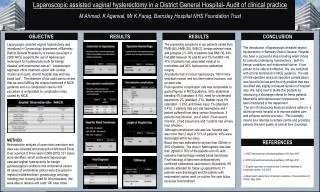
Does Operative Technique of Performing Distal Anastomosis in Acute type A Dissection Affect Early And Late Clinical Outcomes? Sotiris C. Stamou, MD, Ph.D, Nicholas T. Kouchoukos, MD, Robert C. Hagberg, MD, Kamal Khabbaz, MD, Robert M. Stiegel, MD, Mark K. Reames, MD, Eric Skipper, MD, Marcy Nussbaum, MS, Francis Robicsek, MD, Kevin W. Lobdell, MD Divisions of Thoracic and Cardiovascular Surgery Missouri Baptist Medical Center, St. Louis, MO Beth Israel Deaconness Medical Center, Harvard Medical School, Boston, MA Sanger Heart and Vascular Institute, Carolinas Medical Center, Charlotte, NC
Objective To evaluate the early and late clinical outcomes of two different surgical techniques for repair of acute type A dissection: • open distal anastomosis under deep hypothermic circulatory arrest (DHCA) and • distal aortic clamping on moderate hypothermic cardiopulmonary bypass (ACPB)
Acute Aortic Dissection Type A (Stanford) Inspection of the arch for additional intimal tear No Yes Study Group Patient Exclusion ACPB (n=42) DHCA (n=82)
Preoperative Characteristics DHCA ACPB P N (n=82) (n=42) Females 35% 29% 0.55 Diabetes 10% 5% 0.49 Hypertension 83% 81% 0.81 Renal Failure 15% 3% 0.06 Instability 21% 10% 0.18
Operative Characteristics I DHCA ACPB P N (n=82) (n=42) CABG 17% 21% 0.63 Aortic Valve Procedure Resuspension 58% 68% 0.33 Replacement 17% 5% 0.09 Composite root 6% 19% 0.06 Nothing 19% 7% 0.11
Operative Characteristics II DHCA ACPB P N (n=82) (n=42) Arterial Cannulation Axillary a 16% 10% 0.70 Femoral a 76% 83% Other 8% 7% ACP 22% ------ RCP 10% ------ Circ Arrest Time 23+15 <1min <0.001 (Mean/SD) (ACP= Antegrade cerebral perfusion, RCP= retrograde cerebral perfusion)
Postoperative Characteristics DHCA ACPB P N (n=82) (n=42) Reop for Bleeding 20% 34% 0.16 Renal Failure 20% 19% 0.99 Atrial Fibrillation 27% 36% 0.31 Stroke 16% 24% 0.33 Length of Stay 16+13 18+15 0.68 Operative mortality 17% 21% 0.63
Freedom from Death at 5 Years 1.0 DHCA ACPB 0.9 0.8 Death Free Probability 0.7 Log Rank p = 0.99 0.6 0.5 1 2 3 4 5 Time to Death (in years) 30 day 1 year 2 years 3 years 4 years 5 years DHCA (N=42) 34 (81%) 31 (74%) 31 (74%) 31 (74%) 31 (74%) 31 (74%) ACPB (N=82) 67 (82%) 62 (76%) 61 (74%) 60 (73%) 60 (73%) 60 (73%)
Conclusion • No significant differences in operative mortality, major morbidity and actuarial 5-year survival were observed between DHCA and ACPB. • However, there are some practical technical advantages if the distal anastomosis is performed with an open manner • More studies are required to determine the fate of the false lumen and the incidence of dissecting aneurysms with the two techniques.