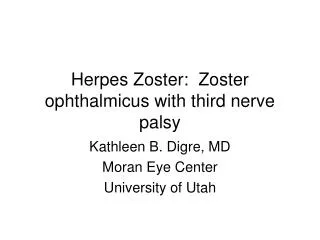
Third Nerve Palsy
946-6. Third Nerve Palsy. History.

Third Nerve Palsy
E N D
Presentation Transcript
946-6 Third Nerve Palsy
History A 50-year old man with type II diabetes presented with a five month history of a flu-like illness characterized by mild fevers, frequent chills, night sweats, sinus congestion, and diffused myalgias in the chest, abdomen, legs and feet. Three days prior to admission (PTA) he awoke unable to open his right eye. With his eyelid open, he saw double.
Concomitantly he experienced decreased auditory acuity, right greater than left, gait imbalance and a dull bifrontal headache. He denied photophobia, phonophobia, stiffness of the neck, vertigo, tinnitus, and ear pain. Several months PTA he had become more serious, pessimistic, and depressed. Three days PTA he became somnolent, lethargic and incoherent with impaired short-term memory and word finding.
The patient takes walks with his dog in the woods and travels frequently in the U.S. No history of drug or alcohol abuse.
Examination Temperature 100.3°, pulse regular, BP 150/80 No neck stiffness No lymphadenopathy or skin rash Oriented x3. Impaired short term memory, 0/3 at 3 min. Naming intact and able to read Pupils: dilated, fixed 7mm OD, 2mm reactive OS EOM: complete 3rd nerve palsy OD
Fundus: normal optic discs OU 8th carnial nerve, decreased hearing to a medium snap bilaterally Limbs: mild right pronator drift and slowness of rigth dextrous movements No finger-to-nose or heel-to-shin ataxia. Gait ataxia and unable to tandem walk Sensory exam intact Reflexes 2+ bilaterally, right plantar equivocal, left flexor
Blood Tests Rapid Plasma Reagin (RPR) test reactive at 1:64 dilution FTA-ABS reactive 1:20 ESR 68 HIV antibody non reactive Serum IgA, IgG (both elevated), IgM normal
Audiogram Moderate to severe sensorineural hearing loss Lumbar Puncture OP 180mm H20, protein 142 mg/dl, sugar 64 mg/dl WBC 755, 27% polys, 56% lymphs IgA, IgG (both elevated), no banding CSF VDRL reactive at 1:2 dilution, RPR reactive at 1:65
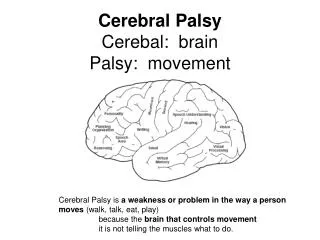
Brian MRI/DWI Acute infarcts in the left anteromedial inferior thalamus extending into the uncus and in the left globus pallidus. No meningeal enhancement. MRA Beaded basilar artery and right PCA > left PCA
Diagnosis Meningovascular syphilis Therapy Penicillin G IV 4 million units q.4h for 14 days
Vasculitis Inflammation of blood vessels that is often accompanied by necrosis and occlusive changes Clinical spectrum complex May occur de novo as a primary disorder or as a secondary manifestation of a diverse group of systemic diseases
Vasculitis May be generalized or localized, clinically silent or have a multitude of symptoms and serious consequences Diagnosis depends on the correct interpretation of histological changes since there are no pathognomonic clinical and laboratory findings