Download
1 / 35
350 likes | 475 Views
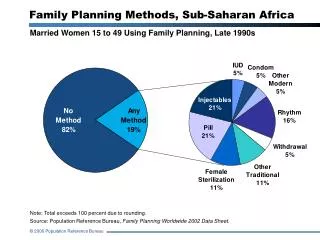
Voluntary, Rights-based Family Planning Framework: What , Why, and How ?. Module 1: Orientation. Agenda. Opening Remarks—[name , title] Ice breaker Presentation: Introduce the VRBFP Framework Discussion Case Studies Discussion Facilitator: [name , title]. Objectives.

E N D
Voluntary, Rights-based Family Planning Framework:What, Why, and How? Module 1: Orientation
Agenda • Opening Remarks—[name, title] • Ice breaker • Presentation: Introduce the VRBFP Framework • Discussion • Case Studies • Discussion Facilitator: [name, title]
Objectives • Explain what a rights-based approach in FP means • Explain why it is important for FP programs to take a voluntary, rights-based approach • Introduce the VRBFP framework and describe how it can be used in programs • Provide a hands-on opportunity to apply the framework using case studies
Human rights are internationally agreed-on entitlements that all people have by virtue of being human. They are articulated in international treaties, conventions, protocols, and other instruments that have the status of international law (i.e., they are legal obligations). Individual human dignity is at the core. What Are Human Rights?
Right to Health: Governments have an obligation to provide health services with the following elements: General Comment 14, Article 12 from the UN Committee on Economic, Social and Cultural Rights. 2000.
3 broad categories of reproductive rights • Rights to reproductive self-determination • Right to bodily integrity and security of person • Rights of couples and individuals to decide freely and responsibly the number and spacing of their children • Right to make decisions concerning reproduction free of discrimination, coercion, and violence • Rights to sexual and reproductive health services, information, and supplies • Including right to the highest attainable standard of health • Rights to equality and nondiscrimination Erdman and Cook (2008)
The rights of individuals and couples: “These (reproductive) rights rest on the recognition of the basic rights of all couples and individuals to decide freely and responsibly the number, spacing, and timing of their children, and to have the information and means to do so…”“ The principle of informed free choice is essential to the long-term success of family planning programmes.” ICPD, 1994 "The human rights of women include their right to have control over and decide freely and responsibly on matters related to their sexuality, including sexual and reproductive health, free of coercion, discrimination and violence.” Beijing Women’s Conference, 1995 Reproductive and human rights re: FP
Respect (refrain from interfering with or curtailing the enjoyment of human rights) Protect (guard against human rights abuses) Fulfill (take action to facilitate the enjoyment of…) …human rights for both clients and potential clients in the way the program is designed, implemented, monitored, and evaluated Rights-based programs…
The status of human rights varies among countries and FP programs. Political, cultural, and resource constraints may hinder some elements of a rights-based approach. Governments and implementers should take whatever steps possible to advance the protection and fulfillment of human rights in their FP programs over time. Incremental steps continue to leave many people vulnerable to human rights violations; sustain advances to gradually realize rights for all. Progressive realization • Checkpoints for Choice, EngenderHealth, 2014
Human Rights Principles (PANEL) ( UNESCO, 2008)
Additional Principles • Voluntary Family Planning (USAID): • The opportunity to choose voluntarily whether to use FP or a specific FP method • Access to information on a wide variety of FP choices • Clients are offered, either directly or through referral, a broad range of methods and services • Verify client’s voluntary and informed consent for sterilization in a written consent document signed by the client • Public Health Programming: • Beneficence • Equity • Autonomy/Agency
WHY? The importance of taking a voluntary, rights-based approach to family planning
Governments have a legal obligation to protect and fulfill the human rights of their citizens. There are practical benefits: both health and rights outcomes benefit both individuals and programs. (HRA contributes to improved health outcomes for women and children, WHO 2013) Rights violations persist in some programs and a human rights-based approach to FP can prevent violations in the future. Why take a rights approach ?
Improves availability, accessibility, acceptability, and quality of family planning information, services, and supplies Ensures voluntarism by protecting the right of the individual to decide freely and responsiblywhether and/or when to have children Expands access to family planning without discrimination or coercion; removes barriers to reach groups not currently being served Demands effective monitoring and accountability mechanisms toidentify and address violations Informs program design or strengthening to ensure respect for individual dignity and promotion of individual agency Practical benefits of a rights-based approach
Violations persist • Coercionin family planning = actions or factors that compromise individual autonomy, agency, or liberty in relation to contraceptive use or reproductive decision making through force, violence, intimidation, or manipulation. Hardee et al., publication pending 2014* • Access barriers prevent many people—particularly the underserved, hard to reach, unmarried youth—from getting the contraception they want.
Coercion in family planning • Excessive social pressure • Targets and performance management indicators linked to numbers of acceptors • Incentives and disincentives • Enforced policies limiting the number of births • Involuntary contraceptive use Hardee et al., publication pending 2014*
Challenges to rights—it’s about more than blatant coercion Subtle Overt Coercion Barriers
Challenges to rights—it’s about more than blatant coercion Subtle Overt Coercion A rights-based approach can address each of these challenges Barriers
Finding common ground A human rights–based approach can enhance both health and human rights outcomes. Checkpoints for Choice, EngenderHealth, 2014
Operationalizing human rights in family planning programs How can we ensure public health programs oriented toward increasing voluntary family planning access and use respect, protect, and fulfill human rights in the way they are designed, implemented, and evaluated?
Framework for Voluntary Family Planning Programs that Respect, Protect, and Fulfill Human Rights INPUTS/ACTIVITIES • Policy Level OUTPUTS OUTCOMES • IMPACT • Service Level COUNTRYCONTEXT • Community Level • Individual Level Citation: Hardee, K., et al. 2013. Voluntary Family Planning Programs that Respect, Protect, and Fulfill Human Rights: A Conceptual Framework. Washington, DC: Futures Group. August 2013
Framework for Voluntary Family Planning Programs that Respect, Protect, and Fulfill Human Rights INPUTS & ACTIVITIES OUTPUTS OUTCOMES IMPACT • POLICY LEVEL • Illustrative • Family planning services are • Available (adequate number of service delivery points, equitably distributed) • Accessible(affordable and equitable; free from discrimination; no missed opportunities for service provision) • Acceptable(respectful of medical ethics, culturally appropriate, and clients’ views are valued) • Highest quality (scientifically and medically appropriate and of good quality (e.g., full, free, and informed decisions; a broad choice of methods continuously available; accurate, unbiased, and comprehensive information; technical competence; high-quality client-provider interactions; follow-up and continuity mechanisms; and appropriate constellation of services) • Accountabilitysystems are in place, which effectively expose any vulnerabilities, and alleged or confirmed rights violations and issues are dealt with in a significant, timely, and respectful manner • Communities actively participate in program design, monitoring, accountability, and quality improvement • Community norms support the health and rights of married and unmarried women, men, and young people and their use of family planning • Agency of individuals is increased to enable them to make and act on reproductive health decisions • Decreased • Unintended pregnancies • Maternal/infant deaths • Unsafe abortions • Adolescent fertility rate • Total fertility rate • Increased • Agency to achieve reproductive intentions throughout the lifecycle • Well-being of individuals, families, communities, and countries • Develop/revise/implement policies to respect/protect/fulfill rights and eliminate policies that create unnecessary barriers to access (All Rs)* • Develop/revise/implement policies to ensure contraceptive security, including access to a range of methods and service modalities, including public, private, and NGO (R2) • Create processes and an environment that supports the participation of diverse stakeholders (e.g. policymakers, advocacy groups, community members) (R2/R3) • Support and actively participate in monitoring and accountability processes, including commitments to international treaties (All Rs) • Guarantee financing options to maximize access, equity, nondiscrimination, and quality in all settings (R2/R3) • Illustrative • Women, men, and young people decide for themselves—free from discrimination, coercion, and violence—whether, when, and how many children to have and have access to the means to do so • Trust in FP programs is increased • Universal access to FP is achieved • Equity in service provision and use is increased • Availability of a broad range of contraceptive methods is sustainable • Women get methods they want without barriers or coercion • FP needs are met; demand is satisfied SERVICE LEVEL • Inform and counsel all clients in high-quality interactions that ensure accurate, unbiased, and comprehensible information and protect clients’ dignity, confidentiality, and privacy and refer to other SRH services (All Rs) • Ensure high-quality care through effective training and supervision and performance improvement and recognize providers for respecting clients and their rights (All Rs) • Ensure equitable service access for all, including disadvantaged, marginalized, discriminated against, and hard-to-reach populations, through various service models (including integrated, mobile, and/or youth-friendly services) and effective referral to other SRH services (All Rs) • Routinely provide a wide choice of methods and ensure proper removal services,supported by sufficient supply, necessary equipment, and infrastructure (R2) • Establish and maintain effective monitoring and accountability systems with community input; strengthen HMIS and QA/QI processes (All Rs) COUNTRY CONTEXT Assess to inform interventions COMMUNITY LEVEL • Engage diverse groups in participatory program development and implementation processes (R2/R3) • Build/strengthen community capacity in monitoring and accountability and ensure robust means of redress for violations of rights (R2/R3) • Empower and mobilize the community to advocate for reproductive health funding and an improved country context and enabling environment for FP access and use (All Rs) • Transform gender norms and power imbalances and reduce community-, family-, and partner-level barriers that prevent access to and use of FP (R3) • Support healthytransitions from adolescence to adulthood (All Rs) * Reproductive rights: R1: reproductive self-determination R2: access to sexual and reproductive health services, commodities, information, and education R3: equality and non-discrimination (“All Rs” indicates that all rights are encompassed) INDIVIDUAL LEVEL • Increase access to information on reproductive rights, contraceptive choices (All Rs) • Empower, through education and trainingabout reproductive health, self-esteem, rights, life-skills, and interpersonal communication (R1/R2) • Foster demand for high-quality services and supplies through IEC/BCC and empower individuals to demand their rights be respected, protected, and fulfilled (R2) August 2013 Citation: Hardee, K., et al. 2013. Voluntary Family Planning Programs that Respect, Protect, and Fulfill Human Rights: A Conceptual Framework. Washington, DC: Futures Group.
Need to partner across sectors, service modes, and disciplines RIGHTS Public sector EDUCATION HEALTH Facility-based services Community-based services Private commercial sector NGOs Social marketing Checkpoints for Choice, EngenderHealth, 2014
Publications Systematic reviews of tools and interventions are summarized in additional publications
Discussion • Questions? • Observations? • What challenges do you envision • Related to what you are already doing—it may not be as difficult as you think.
Build on the good work you are already doing Youth-friendlyservices Access Gender equity
An extraordinary opportunity for voluntary family planning • Pledge of political will and resources with FP2020 • Opportunities offered by the costedimplementation plan development process that is underway • Availability of new tools to apply abstract human rights concepts in actual practice
Case studies (45 minutes) • In your small group, discuss what factors supported or challenged contraceptive choice and human rights in this case study. Write each individual factor on a note card or Post-It and determine the level in the health system at which it exists. • For each challenge identified, consider what should be done to promote respect for, protection, and fulfillment of human rights in the program described. Use one note card or Post-It for each suggested intervention or change. • Select someone at your table to post and explain your cards during the report back.
Discussion • Did anything surprise you? If so, what and why? Is there anything familiar about the circumstances described in the case studies? • Which of the suggested interventions or changes would be relatively easy to implement? • Which might be harder? How might you be able to begin? What more would it take?
Next steps **Tailor this slide to the context of the presentation**