Download
1 / 1
10 likes | 167 Views
No. 165. Robot assisted laparoscopic management of a recto- vesical fistula following laparoscopic radical prostatectomy. R. Thanigasalam , P-E. Theveniaud , A. Hajj, W. Massoud , M. Fennouri , F.Girard , O. Dumonceau , H. Baumert

E N D
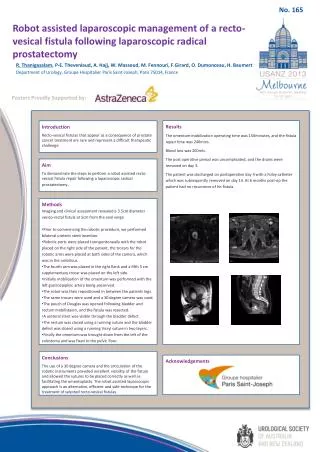
No. 165 Robot assisted laparoscopic management of a recto-vesical fistula following laparoscopic radical prostatectomy R. Thanigasalam, P-E. Theveniaud, A. Hajj, W. Massoud, M. Fennouri, F.Girard, O. Dumonceau, H. Baumert Department of Urology, GroupeHospitalier Paris Saint-Joseph, Paris 75014, France Posters Proudly Supported by: Results The omentum mobilization operating time was 150minutes, and the fistula repair time was 240mins. Blood loss was 200mls. The post operative period was uncomplicated, and the drains were removed on day 3. The patient was discharged on postoperative day 4 with a Foley catheter which was subsequently removed on day 14. At 6 months post-op the patient had no recurrence of his fistula. Introduction Recto-vesical fistulas that appear as a consequence of prostate cancer treatment are rare and represent a difficult therapeutic challenge Aim To demonstrate the steps to perform a robot assisted recto-vesical fistula repair following a laparoscopic radical prostatectomy. • Methods • Imaging and clinical assessment revealed a 3.5cm diameter vesico-rectal fistula at 5cm from the anal verge. • Prior to commencing the robotic procedure, we performed bilateral uretericstent insertion. • Robotic ports were placed transperitoneally with the robot placed on the right side of the patient, the trocars for the robotic arms were placed at both sides of the camera, which was in the umbilicus. • The fourth arm was placed in the right flank and a fifth 5 cm supplementary trocar was placed on the left side. • Initially mobilisation of the omentum was performed with the left gastroepiploic artery being preserved. • The robot was then repositioned in between the patients legs. • The same trocars were used and a 30 degree camera was used. • The pouch of Douglas was opened following bladder and rectum mobilistaion, and the fistula was resected. • A ureteralstent was visible through the bladder defect. • The rectum was closed using a running suture and the bladder defect was closed using a running Vicryl suture in two layers. • Finally the omentum was brought down from the left of the colostomy and was fixed to the pelvic floor. Conclusions The use of a 30 degree camera and the articulation of the robotic instruments provided excellent visibility of the fistula and allowed the sutures to be placed correctly as well as facilitating the omentoplasty. The robot assisted laparoscopic approach is an alternative, efficient and safe technique for the treatment of selected recto-vesical fistulas. Acknowledgements





