Download
1 / 23
240 likes | 256 Views
Resection and Transplantation for HCC in Patients with NAFLD. Julie Heimbach Professor of Surgery Chair, division of transplantation Surgery Mayo Clinic. Outline : Resection Differences in patient characteristics for NAFLD/HCC and non-NAFLD/HCC Outcomes Transplant

E N D
Resection and Transplantation for HCC in Patients with NAFLD Julie Heimbach Professor of Surgery Chair, division of transplantation Surgery Mayo Clinic
Outline: • Resection • Differences in patient characteristics for NAFLD/HCC and non-NAFLD/HCC • Outcomes • Transplant • Incidence and demographics • Outcomes *NAFLD/metabolic syndrome may also be present in setting of ALD, overlap with other etiologies Berot and Adams Expert Reviews GI and Hep 2019
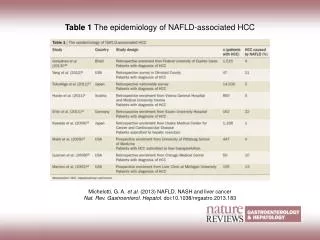
Meta-analysis of case control and cohort studies assessing risk of HCC in patients with DM Diabetes Increases Risk of HCC in Patients With or Without NASH El Serag. Clin Gastro Hep. 2006. 1 Effect p 10 Lower df 0.1 Upper 2.5 2.5 2.5 2.0 2.8 2.1 2.5 1.5 1.8 1.5 1.9 1.3 2.2 1.0 2.1 1.0 2.9 3.1 3.2 3.1 3.7 4.1 3.0 2.4 23 12 11 8 8 6 6 10 <0.01 <0.01 <0.01 <0.01 <0.01 0.02 <0.01 0.26 All Studies (n = 25) Case-Control (n = 13) Cohort (n = 12) US studies (n = 9) European studies (n = 9) Japanese studies (n = 7) Population controls (n = 7) Hospital controls (n = 11) Most studies adjusted for multiple comorbidities, but not always for BMI
Obesity Increases Risk of Primary Liver Cancer in Patients With or Without NASH Chen. Eur J Cancer. 2012. Studies Obesity (BMI >30) RR (95%CI) Moller et al. (1994) Wolk et al. (2001) Nair et al. (2002) Calle et al. (2003) Samanic et al. (2004) Oh et al. (2005) Rapp et al. (2005) Batty et al. (2005) Kuriyama et al. (2005) Samanic et al. (2006) N’Kontchou et al. (2006) Ioannou et al. (2007) Jee et al. (2008) Chen et al. (2008) Ohki et al. (2008) Joshi et al. (2008) Wang et al. (2009) Loomba et al. (2010) Hart et al. (2010) Overall (I-squared = 67.9%, p -0.000) 1.90 (1.50, 2.50) 2.40 (1.60, 3.40) 1.65 (1.22, 2.22) 2.03 (1.69, 2.43) 1.33 (1.19, 1.48) 1.53 (1.06, 2.22) 1.67 (0.75, 3.72) 3.02 (0.80, 11.40) 1.04 (0.51, 2.11) 3.13 (2.04, 4.79) 2.80 (2.00, 4.00) 2.50 (1.30, 4.90) 1.54 (1.26, 1.88) 2.06 (1.22, 3.46) 3.10 (1.41, 6.81) 1.08 (0.67, 1.72) 1.70 (1.02, 2.08) 1.43 (1.03, 1.98) 2.84 (1.34, 6.02) 1.83 (1.59, 2.11) .2 .5 1 2 5
Single-center analysis 1995-2014- French • N=323 patients undergoingresection for HCC • Prevelence of NAFLD increased over studyperiod (2% to 20%) Pais et al, APT 2017
HCC+ NAFLD more likely to be in absence of fibrosis/cirrhosis, and at older age (71 v 51) Prevalence of metabolic risk factors increased in the study period for all pts Pais et al, APT 2017
Etiology of cirrhosis not related to outcome Pais et al, APT 2017
Liver Resection for Nonalcoholic Fatty Liver Disease-Associated Hepatocellular Carcinoma Koh et al JACS 2019 • Two centers, N=844 non-NAFLD HCC versus N=152 NAFLD HCC, Singapore. 2000-2015 • NAFLD pts were older, more often female, and had greater blood loss, LOS, and complications • Superior 5 year outcomes for NAFLD patients (HR=0.67,p=0.04) • Comorbidities (age, CHF, tumor characteristics, Childs B) contributed to worse survival
Yang et al J GastrointSurg 2019 • Multi-center 2003-2011, China • N=1483, undergoing resection for HCC • 96 (6.5%) NAFLD, 1387 (n=93.5%) HBV • NAFLD older, more often female, less likely to have cirrhosis (30% vs 70%), similar survival, similar morbidity before, after PSM
Liver resection for hepatocellular carcinoma in patients with metabolic syndrome: A multicenter matched analysis with HCV-related HCC • Multi-center, Italy 2000-2012, N=1563, with 96 NAFLD HCC matched to HCV patients • Similar peri-operative outcomes– • risk factors: cirrhosis, major hepatectomy, MELD>8 but not NASH • NAFLD had better long term outcome (pre-DAA era) Vigano et al J Hep 2016
Outcomes of Curative Treatment for HepatocellularCancer in Nonalcoholic Steatohepatitis VersusHepatitis C and Alcoholic Liver Disease • N=321, 2000-2010, 52 NAFLD and 168 HCV, ALD single US center • Older (68 vs 59), more often female, less likely to have cirrhosis, • No difference in recurrence free survival but overall survival better in NAFLD Reddy et al Hepatology 2012
Survival after treatment with curative intent for hepatocellular carcinoma among patients with vs without non alcoholic fatty liver disease Wong et al. AP&T 2017 transplant resection NAFLD NAFLD • SEER data, 1991-2011. N=17,664 • NAFLD 46% less likely to be offered curative therapy, but not an predictor of worse survival
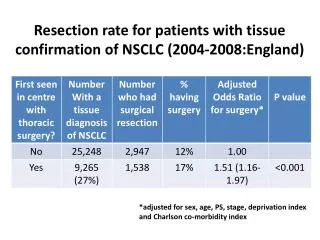
NAFLD more likely to be resected w/o cirrhosis and transplanted with cirrhosis Gawrieh et al AP&T 2019 • 5 US centers, 2000-2014 • N=5144 pts with HCC. 26% had NAFLD • Resection (HR=0.24) and transplantation (HR=0.16) associated with improved survival
Outcomes of LT for NASH: an ELTR study Haldar et al J Hep 2019 NASH
ELTR study continued • 1.4% TX for NASH in 2002 up to 8.6% in 2016. 39.1% of NASH patients had HCC, vs 28.9 % of non-NASH • NASH was not an independent predictor of survival in patients with or without HCC • Causes of death post LT were similar in NASH and non-NASH patients (infection, CV); there was more extra-hepatic malignancy in ALD and recurrent disease in HCV
Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates • SRTR 2002-2016 • N=158,000: HCC rose from 6.4% in 2002 to 23% in 2016 • HCV is still most common cause for HCC, NASH rising faster and is currently second. • HCC recurrence is lowest in NASH, highest in HBV Younossi et al CGH 2019
2004-2014, UCSF and University of Toronto, N=929 transplanted for HCC, 60 for NASH • NASH patients were older, and had more females (38% vs 18%) • Tumors characteristics were similar (size, number, microvascular invasion) • Outcomes similar Sadler et al Transplantation 2018
Comparison for beyond Milan only, favored NASH patients (n=19) • Higher proportion of NASH had microvascular invasion, yet still had more favorable outcome • ? Unknown whether NASH related tumors inherently less aggressive Sadler et al Transplantation 2018
Impact of obesity on outcome of LT for HCC? Siegel et al Transplantation 2012 • Single center, US N=342 LT for HCC. 1999-2010 • BMI>30 associated with increased risk of death, microvascular invasion, and HCC recurrence
Impact of obesity on outcome of LT for HCC? Ata et al HPB 2019 • UNOS data N=8352 LT for HCC • 2002-2013 • Donor and recipient BMI
Future Trends in Demand for Liver Transplant: Birth Cohort Effects Among Patients With NASH and HCC Shingina et al Transplantation 2019 • Rates of obesity in US are 39.8% of adults and 18.5 % of children • Analysis of birth cohorts to determine future trends in LT registration due to NASH, with and without HCC
Future Trends in Demand for Liver Transplant: Birth Cohort Effects Among Patients With NASH and HCC Shingina et al Transplantation 2019 Observed LT registration by age group in NASH patients Observed and projected LT registration for NASH+HCC
Summary • HCC-NAFLD resection patients tend to be older, more often female, more metabolic disease, less cirrhosis, with similar tumor characteristics and similar outcomes • HCC-NAFLD transplant patients also older, more female, similar outcomes. Obesity not likely to impact outcome for selected patients. Rising indication for LT