Download

1 / 64
1.31k likes | 2.78k Views
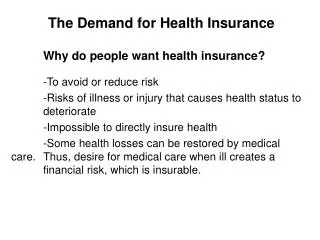
Demand for Health Care. Production Function for Health. Health = H(medical care, other inputs, time). Health Status. H. H 2. H 1. Iatrogenic disease. M 1. M 2. M 3. Medical Care Spending. Health Status Measurements. Mortality: probability of death

E N D
Production Function for Health • Health = H(medical care, other inputs, time) Health Status H H2 H1 Iatrogenic disease M1 M2 M3 Medical Care Spending
Health Status Measurements • Mortality: probability of death • Morbidity: probability of illness/disability • Quality of life: QALY
Health Status Determinants Health = H(medical care, other inputs, time) • Income and education • Environmental and lifestyle factors • Diet, exercise, sexual behavior, substance abuse, violence • Genetic factors • The role of public health • Immunization, clean air/water, food handling
$ Q Demand for Medical Care • Demand Function • Health status:acute/chronic care • Demographic characteristics:age, gender, population • Economic standing • Physician factors QMC = M(P; HS, DC, ES, PF)
Effect of Insurance on Demand D100% Price D50% D0% P0 ½ P0 Q0 Q1 Q2 Medical Care
Physician Induced Demand • S & D may not be independent due to principal-agent problem • Graphical story • Empirical evidence is mixed • Fuchs and Kramer (1986): # of physicians and fees are positively correlated • Reinhardt (1985): physicians migrate to high fee areas
Estimating Demand • Problem Set #8 • Price elasticity of demand E = %ΔQ %ΔP • Income elasticity of demand E = %ΔQ %ΔM
RAND Experiment: 1974-82 • Randomly assigned 2,000 non-elderly families to insurance plans differing in 2 characteristics: • Coinsurance rate: 0, 25%, 50%, 95% • Annual spending cap of $1,000 • Examined 2 measures: • Health spending • Health outcomes
RAND Experiment Spending • Research question: How did assignment to groups affect spending?
Data from Manning WG et al. 1987. “Health insurance and the demand for medical care: Evidence from a randomized experiment.” American Economic Review, 77(3):251-277.
RAND Experiment Spending • Research question: How did assignment to groups affect spending? • Economic lesson: increase the price and reduce the amount consumed
RAND Experiment Health Outcomes • Study question: How did assignment to groups affect outcomes? • For average person – no substantial health benefits from free care • Exception: poor and chronically ill did better with free care (hypertension, vision, dental care)
RAND Experiment Conclusions • Instead of free for all care: • Targeted benefits for chronic conditions • Exempt low-income from cost sharing • Study changed policy debate • Cost sharing limits demand without substantially harming health
Social insurance Medicare Medicaid Indemnity insurance Provides reimbursement for expenditures or loss of income Premiums (price) reflects expected loss (cost) Types of insurance • Hospitalization • Physician services • Major medical • Dental • Disability income protection • Long-term care
Insurance Theory • People prefer to avoid risky outcomes • May be willing to pay to avoid risky outcomes
Utility when healthy PH = probability of being healthy PS = probability of being sick Expected Utility without insurance PH + PS = 1 Utility when sick Expected Utility Theory Assumes diminishing marginal utility of income Utility U 90 86 E(U) = PHU($40,000) + PSU($20,000) = PH•90 + PS•70 Let PS = .20 E(U) = (.80)90 + (.20)70 = 86 E(Y) = (.80)(40,000) + (.20)(20,000) = $36,000 70 Income (thousands) $20 $36 $40 Medical illness costs $20,000
Utility from a certain income of $35,000 Expected Utility Theory Utility U 90 86 Paying $5,000 to insurer leaves consumer with 86 utils, which equals E(U) without insurance. 70 Loading fee Expected medical costs Income (thousands) $20 $35 $36 $40
Determinants of HI Demand • Price of insurance • In the previous example, the consumer will forego health insurance if the premium is greater than $5,000. • Degree of Risk Aversion • Greater risk aversion increases the demand for health insurance. • Income • Larger income losses due to illness will increase the demand for health insurance. • Probability of Illness • Consumers demand less insurance for events most likely to occur (e.g. dental visits). • Consumers demand less insurance for events least likely to occur. • Consumers more likely to insure against random events.
Health Insurance and Market Failure • Income tax treatment • Information problems • Moral hazard • Adverse selection • Free riders
Tax Subsidy • Employer-paid health insurance is exempt from federal, state, and Social Security taxes • Employee will prefer to purchase insurance through work, rather than on his own.
Employee Purchased Income $1,000 28% tax <280> after tax 720 insurance <50> net pay 670 Employer Purchased Income $1,000 insurance <50> subtotal 950 28% tax <266> net pay 684 Example: Cost of insurance when income is $1,000 per week and income tax rate is 28% $50 weekly insurance premium
Adverse Selection • Occurs because one party to a contract has more information than the other • Too many high risk users contaminate the risk pool; drives premiums up • Creates incentives for low risk users to drop out
Moral Hazard • Occurs when one party to a contract cannot monitor the other party’s performance • Insured people engage in more risky behavior • Insured people are likely to spend more on health care The Peltzman Effect
Insurers’ Response to Market Failure • Response to overspending: • Deductibles • Coinsurance • Response to adverse selection: • Require physical exams • No preexisting conditions will be covered
Efficient Pooling? • Experience rating • Community rating • Cream skimming • Self-insurance
Managed Care • Contractual arrangements that integrate financing and delivery of medical care • Prepaid health plans (Prospective payment) • Limited benefits • Risk-sharing arrangements
Sidney Garfield and Henry Kaiser History of Managed Care • Kaiser Permanente • Largest non-profit HMO • 8.7 members • 156,000 employees • 13,700 physicians • 37 medical centers • 400 medical offices • HMO Act (1973) • Subsidies to non-profit groups to start HMOs
Types of Managed Care Plans • Health maintenance organizations (HMO) • Group model • Staff model • Network model • Preferred provider organizations (PPO) • Similar to network model except enrollees can go outside network • Point-of-Service plans (POS) • Hybrid of HMO and PPO
“gatekeeper” Managed Care Cost Savings: Theory • Selection of providers • gatekeepers • Cost sharing arrangements • Capitation for general practitioners • Risk-sharing contracts • Bonuses • Withholdings • Practice guidelines and utilization review • “evidence-based” medicine plans • Pre-authorization • Second-opinions • Hospitalists
Managed Care Cost Savings: Evidence • RAND (Manning et al,. 1984): per capita costs 28% lower under HMO due to fewer hospital admissions and shorter stays • Miller and Luft (1994, 1997): HMO cost savings of 10-15% due to shorter hospital stays, fewer tests, less costly procedures • Glied (1999): overall evidence inconclusive since managed care attracts healthier enrollees
Managed Care Quality: Evidence • Miller and Luft (1997) and Robinson (2000): found mixed evidence on overall quality differences • Ware et al. (1996), Robinson (2000), and Hellinger (1998): poorer outcomes among members of vulnerable subpopulations—sick, elderly, poor
Managed Care and Its Public Image • Considerable economic success • Cultural and political failure • Patient/Provider Backlash • Patient rights • Humana law suit • cost-based criteria rather than medical-need
The Future of Managed Care • Patients – Model too restrictive • Employers – Concerned over litigation prospects, disgruntled employees • Payers – Discovered cost control is unpopular and dangerous to corporate survivability • Providers – Risk sharing is risky. Balking at dual role of agent of patient (associated concern with quality) and agent of society (associated concern with costs)
A New Direction • Consumer driven health care – build on tradition of individual autonomy and cost conscious consumers • Complementary medicine • Informed consent • Expanding use of Internet • Direct-to-consumer advertising • Employer desire to get out of the health care business • Public distrust for government-run programs
Market for Health Care Professionals Physicians Nurses Dentists
Labor Market Theory • Competitive Model • Hiring Rule: MRP = w • Imperfectly Competitive Model • Barriers to entry • Imperfect information • Third-party payment S1 Wage W1 D1 = MRP1 L1 Physicians
Human Capital Model • Medical degree as an investment $ Med Degree Benefits BA Degree Foregone Income Age Direct Cost
Human Capital Model • Investment Rule: invest if PV of Net Benefits > 0 Can solve for internal rate of return for which NB = 0 Mincer Earnings Equation: lnY = β0 + β1S + β2X + ε
Estimated Rates of Return Source: Weeks, Wallace, Wallace, and Welch. “A Comparison of the Educational Costs and Incomes of Physicians and Other Professionals,” New England Journal of Medicine 330(18), 1994. Problem Set #30