Download
1 / 12
1.03k likes | 5.17k Views
Clinical Case Presentation: Alcoholic Liver Disease. Gaurav Jain Roll No: 174/11. Clinical Case Presentation: Ascites with ARF. Lakshmi Narayan, 42 years old patient , who is a chronic alcoholic , farmer by occupation presented with: Abdominal distension from 15 days

E N D
Clinical Case Presentation: AlcoholicLiver Disease Gaurav Jain Roll No: 174/11
Clinical Case Presentation:Ascites with ARF • Lakshmi Narayan, 42 years old patient , who is a chronic alcoholic, farmer by occupation presented with: • Abdominal distension from 15 days • Abdominal pain from 15 days • Fever from 15 days • Decreased urine output from 10 days • Decreased passage of stools from 10 days
HISTORY • H/O Present illness: • HDBT 15 days when patient developed: • insidious, gradually progressive Abdominal distension a/w pin-pricking pain in the epigastrium & right hypochondrium region , relieved by medication. • Intermittent, mild to moderate grade fever, insidious onset & subsides on medication a/w nausea ,retching, cachexia, altered sleep patterns with day-time sleepiness. • Pt. developed decrease in urine output without burning or other discomfort from past 10 days. • Pt. developed decreases stool passage ,insidious onset and gradually progressive, not a/w flatulence, dyspepsia, heart burn from 10 days. • A single episode of haemetemesis containing 30 ml of fresh blood.
Negative History: No H/Ochills, rigor, sweating,headache,rashes retrobulbar pain, cough, joint pain, steatorrhea, malena, facial puffiness, xanthelasma, xanthomata, flapping tremors, blood transfusion. • Past History: No H/O TB, Diabetes, Asthma, Hypertension. No such complaint in the past. • Personal History: Married with two children • Non vegeterian diet. • Smoking-15 pack years but one bundle daily from past 2 months. • Chronic alcoholic from past 30 years consuming 4.5-5.6 units of alcohol daily. Tobacco chewing from past 12 years. • Lost 15 kgs of weight in past 2 months. • Family History: No such family history. • Drug History: No significant history.
EXAMINATION • General Physical Examination • Patient is conscious, oriented to time,place and person and cooperative. • No pallor, icterus, cyanosis, clubbing, JVP and lymphadenopathy. Pedal edema present. • No gynaecomasatia, skin pigmentation , palmar erythema, spider nevi, leuconychia, koilonychia, angular stomatitis present. • Axillary ,pubic hair decreased. Mild Glossitis present • PR- 86/min RR-20/min BP-96/60mmHg • Abdominal Girth: 114.3 cm • Umblico-ischial spine distance: 19.05 cm • Umblico-Symphysis distance: 21.59 cm
Abdominal Examination • Inspection: globular shape stomach with full flanks and everted umblicus. There is a single scar present on the right lateral side. Engorged veins seen.(downward to upward blood • flow). • Palpation: afebrile .Liver not palpable. Spleen palpable by Dipping method but size cant be established. Fluid thrill present. . Tense and tendor • Percussion: Shifting Dullness present. • Auscultation:Bowel sounds heard and Bruits not heard. • Other systemic findings were normal.
INVESTIGATIONS HIV, Hep B, Hep C-negative
Complete Urine Examination: Within normal limits. Ultrasonography
Differential Diagnosis: • Based on clinical, lab & USG findings, patient is suffering from Chronic Liver Disease showing complications of Ascites and Portal Hypertension with derangement of KFT, cause of which can be 1) Hepato-Renal Syndrome 2) Pre –Renal Azotemia • High SAAG in the case indicates presence of Portal Hypertension. • Low Ascitic Protein (1.5g/dl) indicates Transudative Ascites. • Based on patients alcoholic history & lab findings,Cirrhosis is the cause of Ascitis and Portal Hypertension. • Complete Urine Analysis within normal limit shows that Chronic Kidney Disease is not the cause of acute renal failure. • Hereditary causes of Cirrhosis are ruled out based on family history while patient gives no history of skin pigmentation,xanthoma and jaundice which rules out Biliary Cirrhosis.
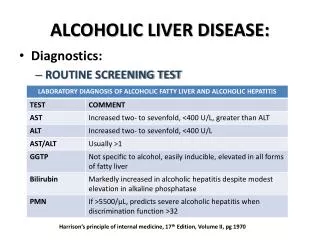
Alcohol Liver Disease • Chronic alcohol ingestion is one of the major causes of liver disease. • It causes 3 major lesions: a)fatty liver b)alcoholic hepatitis c)cirrhosis • Quantity and Duration of alcohol intake are the major risk factors.160g/d for 10-20 years in man produces cirrhosis. • Hepatic metabolism of alcohol initiates a process that promotes lipogenesis& the inhibition of fatty-acid oxidation. Endotoxins, oxidative stress, immunologic activity, and pro-inflammatory cytokine release contribute to the resulting liver injury. • Alcoholic fatty liver and hepatitis is reversible with alcohol abstention but cirrhosis is not. • Diagnosis is based on AST, ALT, GGTP, Bilirubin and USG findings.
A discriminant function can determine patients with poor prognosis.(>32) • The presence of ascites, variceal hemorrhage, deep encephalopathy, or hepatorenal syndrome predicts a dismal prognosis. • Management • Lifestyle modifications: decreased alcohol intake, smoking obesity • Appropriate nutrition/nutritional support • Use of pentoxifylline or prednisone for alcohol hepatitis • Advice on complementary & alternative medicine for cirrhosis(eg silymarin) • Transplantation in selected abstinent patients with severe disease.