Download
1 / 78
780 likes | 867 Views
Advances in the Medical Management of Peripheral Arterial Disease. Warner P. Bundens, MD, MS Associate Clinical Professor of Surgery Associate Clinical Professor of Family and Preventive Medicine School of Medicine University of California, San Diego La Jolla, California. ?.

E N D
Advances in theMedical Management of Peripheral Arterial Disease Warner P. Bundens, MD, MS Associate Clinical Professor of Surgery Associate Clinical Professor of Family and Preventive Medicine School of Medicine University of California, San Diego La Jolla, California
? Key Question How many of your patients with CV risk do you test for peripheral arterial disease? • 0%-24% • 25%-50% • 51%-75% • 76%-100% Use your keypad to vote now!
Faculty Disclosure • Dr Bundens: grants/research support:sanofi-aventis Group.
Learning Objectives • Describe the prevalence and disease burden of PAD • State medical treatments for improving leg symptoms of the patient with PAD • Discuss interventions used to prevent systemic complications in the patient with PAD PAD = peripheral arterial disease.
Peripheral Arterial Disease: What Is It? PAD PAOD PAOD = peripheral arterial obstructive disease.
ObstructedLumen Plaque What Is It? Lesions
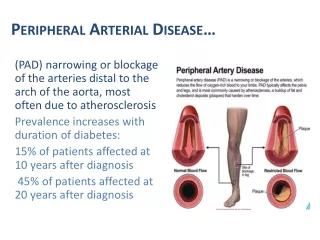
Who Gets It? PAD: Risk Factors • Age • Uncommon: <50 years old • 50-70 years old • 10% overall • 20% with history of smoking or diabetes • >70 years old • 20%
Who Gets It? PAD: Risk Factors • Age • Diabetes 4× • Smoking 3.5× • Past or present • Hypertension 2× • Hyperlipidemia 0.1×
How Do You Diagnose It? PAD Symptoms • May be asymptomatic • Claudication
Claudication A Reproducible and Consistent Symptom
Claudication • Muscular pain brought on by activity (walking) that is relieved by stopping that activity
Claudication • Muscular pain brought on by activity (walking) that is relieved by stopping that activity • Does not occur at rest • Is not brought on by standing
Other Causes of Leg Pain: “Pseudoclaudication” • Spinal stenosis • Nerve root compression • Arthritis/joint disease, especially the hip • Compartment syndrome • Venous claudication • Symptomatic Baker’s cyst
How Do You Diagnose It? PAD Symptoms • May be asymptomatic • Claudication • Ischemic rest pain
Ischemic Rest Pain • Distal foot • Worse at night • Decreased by lowering foot
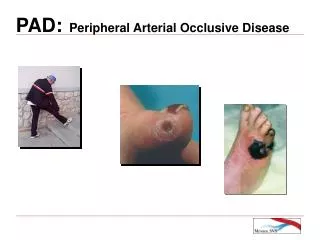
How Do You Diagnose It? PAD Symptoms • May be asymptomatic • Claudication • Ischemic rest pain • Tissue loss, nonhealing lesions, gangrene
Not Arterial Nocturnal Leg/Foot Cramps
PAD: Physical Findings • Pulses • Pallor • Dependent rubor • Thick nails • Hairlessness • Tissue loss/ulcer/gangrene
PAD: Physical Findings Poor Sensitivity and Specificity for Mild-to-Moderate PAD
PAD: An Objective Test Flow vs Pressure
Ohm’s Law Electrical: E = I·R Voltage Drop = Current × Resistance Fluids: P = F·R Pressure Drop = Flow × Resistance
Office Measurement ofthe Ankle-Brachial Index (ABI) Supine Patient Right arm pressure Left arm pressure Pressure: Posterior tibial Anterior tibial Pressure: Posterior tibialAnterior tibial
Ankle Pressure Patient Must Be Supine Posterior Tibial Anterior Tibial
Ankle Systolic Pressure Brachial Artery Systolic Pressure ABI= The ABI • Both ankle and brachial systolic pressures should be taken using a hand-held Doppler instrument • For arm and leg, use higher of 2 pressures
The ABI Right Arm 150 mm Hg Right AT 68 Right PT 75 Left Arm 143 Left AT 120 Left PT 100 Right ABI = 75/150 = 0.50 Left ABI = 120/150 = 0.80 AT = anterior tibial; PT = posterior tibial.
What Do the Numbers Mean? ABI • Typical values • Normal = 1.25-0.9 • Claudication = 1.0-0.3 • Rest pain = <0.4 • Tissue loss = <0.3
ABI <0.90 95% Sensitive and 99% Specific for PAD ? TASC Working Group. J Vasc Surg. 2000;31(1 suppl):S1-S296.
ABI 1.0-0.9 Most of these people have PAD ABI >1.0 Most of these people do not have PAD ABI: Occasional “Gray” Areas
ABI Workshops • Demonstrations available throughout the day
Further Noninvasive Testing • Segmental pressures • Doppler waveforms • Exercise test
Further Testing Lower Extremity Arterial Exam
PAD Is a Bad Disease Relative 5-Year Mortality Rates *American Cancer Society. Cancer Facts and Figures,2000. Criqui MH et al. N Engl J Med. 1992;326:381-386.
? Key Question Without intervention, what percentage of PAD patients will have an MI or stroke in the next 5 years? • 10% • 25% • 50% • 75% Use your keypad to vote now! MI = myocardial infarction.
Clinical Outcomes in Patients With PAD PAD Patient Asymptomatic 50% Intermittent claudication 40% Critical leg ischemia 10% Cardiovascular morbidity/mortality PAD outcomes (5-year outcomes) Stable claudication 73% Worsening claudication 16% Leg bypass surgery 7% Major amputation 4% Nonfatal events (MI/stroke) 20% Mortality 30% Adapted from Weitz Jl. Circulation. 1996;94:3026-3049.
PAD and All-Cause Mortality* 1.00 Normal subjectsAsymptomatic LV-PAD†Symptomatic LV-PAD†Severe symptomatic LV-PAD† 0.75 0.50 Survival 0.25 0.00 0 2 4 6 8 10 12 Year *Kaplan-Meier survival curves based on mortality from all causes. †Large-vessel PAD Adapted from Criqui MH et al. N Engl J Med. 1992;326:381-386.
Treatment Diagnosis 2 Problems Cardiovascular Risk Leg Symptoms Claudication Rest Pain Tissue Loss
Treatment Cardiovascular Risk • Stop smoking • Program • Toes vs cigarettes • Blood pressure control • 140/90 mm Hg • 130/80 mm Hg if patient has diabetes or renal disease • Lipid control • LDL <100 mg/dL • Diabetes control • HbA1C <7% • Antiplatelet medication Hirsch A et al. J Am Coll Cardiol, 2006;47:1239-1312.
Antiplatelet Medications • Aspirin
? Key Question What is the proper daily dose of aspirin for cardiovascular risk reduction? • 75 mg • 81 mg • 300 mg • 325 mg Use your keypad to vote now!
Antiplatelet Medications • Aspirin 81 mg/d
Antiplatelet Medications Aspirin Dosage Aspirin Dose No. Trials OR (%) OR 500-1500 mg 34 19 160-325 mg 19 26 75-150 mg 12 32 <75 mg 3 13 Any aspirin 65 23 0 0.5 1.5 1.0 2.0 Antiplatelet Better Antiplatelet Worse OR = odds ratio. Antithrombotic Trialists’ Collaboration. BMJ. 2002;324:71-86.
Antiplatelet Medications Aspirin Dosage: Risk of Major Bleeding Clopidogrel + Aspirin Placebo + Aspirin Aspirin Dose <100 mg 3.0% 1.9% 100-200 mg 3.4% 2.8% >200 mg 4.9% 3.7% CURE Trial. Circulation. 2003;108:1682-1687.
Antiplatelet Medications • Aspirin • 81 mg • Clopidogrel • 75 mg
CAPRIEClopidogrel vs ASA: MI, Ischemic Stroke, or Vascular Death 16 8.7% Overall RRR (P = .045)* Clopidogrel ASA 5.83% 12 5.32% (N = 19,185) 8 Cumulative Event Rate (%) Subjects had a recent MI, recent ischemic stroke, or symptomatic PAD 4 0 0 3 6 9 12 15 18 21 24 27 30 33 36 Months of Follow-up Median follow-up = 1.91 years *ITT analysis ASA= aspirin; CAPRIE = Clopidogrel vs Aspirin in Patients at Risk of Ischemic Events; RRR = relative risk reduction. CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.
CAPRIE Subgroup Analysis No. Patients Patient with stroke 6431 Patient with MI 6302 Patient with PAD 6452 All patients 19,185 -40 -30 -20 -10 0 10 20 30 40 ASA Better Clopidogrel Better Risk Reduction (%) CAPRIE Steering Committee. Lancet. 1996;348:1329-1339.
PAD Treatment Leg Problems • Asymptomatic • No specific treatment • Claudication • Do nothing