Download
1 / 56
560 likes | 677 Views
Coronary MDCTA Applications. Thomas H. Hauser MD, MMSc, MPH, FACC Director of Nuclear Cardiology Beth Israel Deaconess Medical Center Assistant Professor of Medicine Harvard Medical School Boston, MA. Outline. Possible indications for coronary MDCTA How to approach a coronary MDCTA study.

E N D
Coronary MDCTA Applications Thomas H. Hauser MD, MMSc, MPH, FACC Director of Nuclear Cardiology Beth Israel Deaconess Medical Center Assistant Professor of Medicine Harvard Medical School Boston, MA
Outline • Possible indications for coronary MDCTA • How to approach a coronary MDCTA study
Outline • Possible indications for coronary MDCTA • How to approach a coronary MDCTA study
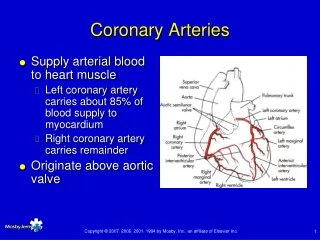
Coronary artery CAD/Plaque Stents Grafts Anomalous coronaries Ventricular size and function Valve imaging Myocardial perfusion Infarct imaging Cardiac vein imaging Congenital heart disease Cardiac masses Cardiomyopathy Pulmonary vein imaging Possible Indications for Cardiac CT
Detection of CAD Accuracy investigators, RSNA 2007
Multi-Center Trial: 16-Slice MDCT Garcia, M. J. et al. JAMA 2006;296:403-411.
Multi-Center Trials: CORE-64, Accuracy • CORE-64 reported at AHA 2007 (Toshiba) • 291 patients at 9 institutions • Sensitivity 85% • Specificity 90% • Excluded patients with calcium score >600 • ACCURACY reported at RSNA 2007 (GE) • 229 patients at 16 institutions • Sensitivity 93% • Specificity 82%
ACCURACY Trial J Am Coll Cardiol Budoff et al. online only
Limitations of Coronary CTA • Coronary Motion • Slab artifacts • Ventricular Ectopy • Ventilatory Motion • Calcium • Stents • Radiation Dose
Coronary Motion Hoffmann et al, J Nucl Med 2006; 47:797–806
Higher Heart Rate = More Motion Hoffmann, M. H. K. et al. Radiology 2005;234:86-97
Slab Artifact Hoffmann et al, J Nucl Med 2006; 47:797–806
Calcium Hoffmann et al, J Nucl Med 2006; 47:797–806
Calcium Raff et al, J Am Coll Cardiol 2005;46:552–7
Stents Gaspar, T. et al. J Am Coll Cardiol 2005;46:1573-1579
Grafts Vessels Segments Sens Spec Grafts 109 182 99% 96% Run-off 109 123 89% 93% Non-BP 116 288 97% 86% Malagutti et al. Eur Heart J 2006 epub
Radiation Dose: High Einstein et al, JAMA. 2007;298:317-323.
Radiation Dose J Am Coll Cardiol Maruyama et al. 52 (18): 1450
Radiation Dose J Am Coll Cardiol Maruyama et al. 52 (18): 1450
Problems Correlating with Angiography • Angiographic stenosis is not perfectly correlated with functional significance • Potential advantages for combining with functional imaging • Identification of non-obstructive plaque may identify patients at increased risk for adverse events • Ongoing prospective studies of prognosis
Angiographic vs. Functional Stenosis Meijboom et al, J Am Coll Cardiol, 2008; 52:636-643
Outcomes after CTA Ostrom et al, J Am Coll Cardiol, 2008; 52:1335-1343
Plaque Characterization Leber et al, J Am Coll Cardiol, 2005; 46:147-154
Anomalous Coronary Arteries http://bhavin.typepad.com/cardiac_images/
Anomalous Coronary Arteries http://bhavin.typepad.com/cardiac_images/
Ventricular Function: Compared to CMR Segung et al, Circulation 2006;114:654-661; 31 patients
Ventricular Function: Compared to CMR Segung et al, Circulation 2006;114:654-661; 31 patients, radial method
Valvular Function http://bhavin.typepad.com/cardiac_images/
Valvular Function http://bhavin.typepad.com/cardiac_images/
Aortic Stenosis Pouleur et al, Radiology 2007;244:745-754
Aortic Stenosis Pouleur et al, Radiology 2007;244:745-754
Aortic Stenosis Agreement between multidetector CT and TTE in the detection of normal (AVA 2 cm2), mildly stenotic (AVA 1.2 cm2 and < 2.0 cm2), moderately stenotic (AVA 0.8 cm2 and < 1.2 cm2), or severely stenotic (AVA < 0.8 cm2) aortic valve opening was excellent ( = 0.88, P < .001) Pouleur et al, Radiology 2007;244:745-754
Perfusion and Late Enhancement Nieman et al. Radiology.2008; 247: 49-56
Perfusion and Late Enhancement Nieman et al. Radiology.2008; 247: 49-56
Perfusion and Late Enhancement Nieman et al. Radiology.2008; 247: 49-56
Cardiac CT • Possible indications for coronary MDCTA • How to approach a coronary MDCTA study
How to Review a Coronary CTA Study • Review the axial images • Interrogate multiple reconstructions at different points in the cardiac cycle to determine which has the least amount of artifact • If any abnormalities, further investigate them with MIPs MPRs, and curved MPRs. • Volume rendered images can be helpful to communicate your findings • Generally not diagnostic • Especially helpful in graft cases • The entire dataset beyond the heart needs to be reviewed to ensure that there are no other significant findings.