Download
1 / 31
330 likes | 833 Views
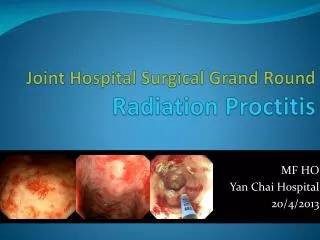
Joint Hospital Grand Round Radiation Proctitis. Nancy Ng Colorectal Team Department of Surgery Prince of Wales Hospital The Chinese University of Hong Kong. Why Important ?. Increasing no. of patients treated with radiotherapy for pelvic malignancies, mostly with curative intent.

E N D
Joint Hospital Grand RoundRadiation Proctitis Nancy Ng Colorectal Team Department of Surgery Prince of Wales Hospital The Chinese University of Hong Kong
Why Important ? • Increasing no. of patients treated with radiotherapy for pelvic malignancies, mostly with curative intent. • 12000 in UK annually • Rectum commonly injured • Acute radiation toxicity : up to 80% • Self-limiting and resolve after RT
Chronic radiation rectal bleeding • Occur 29-51% of patients • Not entirely dose related • Depends on physical, patient-related, treatment and genetic factors • Dearnaley D et al. Lancet 1999 • Widmark A et al. Cancer 1994 • Crook J et al. Urology 1996 • Impaired QOL in 5% • Gami B et al. Aliment Pharmacol Ther 2003 • Manifest from months to years after RT • median 8-13 months
Histopathologic changes • Progressive obliterative endarteritis and submucosal fibrosis • Mucosal ischaemia • Neo-vascularization • Hasleton PS et al. Histopathology 1985 • Haboubi NY et al. Am J Gastroenterol 1988
Diagnosis • Usually straightforward from history • ? Endoscopy : Yes • Older patient and prior pelvic radiation • Increased risk of malignancy, esp. rectal tumor • Pickles, Phililips, et al. Radiother Oncol 2002 • Brenner A, Curtis R, et al. Cancer 2000 • Kleinerman R, Boice J, et al. Cancer 1995 • Boice J, Day N, et al. Cancer Inst 1985 • Other pathologies • H R T Williams, P Vlavianos, et al. Ali Phar & Thera 2005
Treatment • Medical therapy • Oral and rectal steroid • 5-aminosalicylates • Sucralfate • Short chain fatty acid enema • Ineffective in severe cases • Denton AS et al. Br J Cancer 2002 • Hong JJ et al. Aliment Pharmocal Ther 2001 • Tagkalidis PP et al. ANZ J Surg 2001
Treatment • Endoscopic treatment • Local formalin application • Surgical treatment • Rarely response to colostomy alone • High morbidity and mortality • Tagkalidis PP et al. ANZ J Surg 2001 • Hong JJ et al. Aliment Pharmocal Ther 2001 • Indicated for uncertain diagnosis and complications
Endoscopic treatment • Coagulation can be achieved by • heat probe • multipolar electrocoagulation • laser • argon plasma coagulator (APC)
APC • monopolar therapy, use argon gas to conduct radiofrequency energy to tissue • Instant superficial tissue coagulation over 3-4mm area • Non-contact nature minimize tissue sticking and bleeding • Require adequate colon cleansing • Deep injury include perforation can occur (depends on contact time and total energy delivered
PWH experience • From 1/2001 to 12/2004 • 20 (M:4, F:16) with radiation proctitis were treated by endoscopic APC in our hospital • Ca prostate : 4 • Ca rectum : 1 • Gyn malignancy : 15 • Age 67.6 (+/-11.5) years
Radiation dosage : 6300 (+/-1197cGy) • Onset of PRB : 15 mth • Hb before treatment : 10.02g/dl (+/-2) • 6 of them need repeated admission for transfusion
Result • Mean treatment session : 1.5 (1-4) • Bleeding stopped 7 35% • Bleeding improved 5 25% • Bleeding unchanged 6 30% • Bleeding worsened 2 10% • Treatment efficacy : 60% • Hb after treatment : 10.05g/dl (+/-2) • No documented complications
Conclusions • APC is a safe treatment modality for radiation proctitis • Good result from literature not reproduced
Topical Formalin • Formaldehyde mixed with methanol • Treatment for radiation cystitis since 1976 • First described by Rubinstein et al in 1986 • Mechanism • Chemical cauterization by protein cross-linking, cell necrosis and vessel sealing. • Effect of 4% formalin was transient and confine to the mucosa • Myers et al . Dis Colon Rectum 1998
PWH experience • From 1/2001 to 12/2004 • 11 ( M:2, F:9) patient with refractory radiation proctitis failed to medical (11) and /or argon plasma coagulation (7) were included • Age 62.8 (+/-14.8) • Radiation dosage 6723.6 (+/-980cGy) • Ca prostate : 2 • Gyn. malignancy : 8 • Buttock sarcoma : 1
Onset of PRB after RT : 10.9mth(+/-3.8) • Hb before treatment : 7.3g/dl(+/-2.4) • 8 need repeated admission for transfusion • Treatment was done in minor operating theater without anaesthesia or sedation
4% formalin solution was prepared by mixing 40ml of 10% buffered formalin
Patient in left lateral position. Contact for 1 to 3min, till mucosa appears whitish and bleeding stops.
Immediately after treatment Before treatment 4 days later 11 days later 5 weeks later 4 months later
Result Overall efficacy 90.9%
Result • Hb after treatment : 10.4g/dl (+/-2.2) • P = 0.007 • No major complications documented • Conclusion • Formalin dab is an effective, safe and inexpensive treatment modality for refractory radiation proctitis.
Summary • Radiation proctitis is one of the common cause of PRB • Colonoscopy is suggested before making this diagnosis • APC is safe but may not be effective for severe bleeding • Formalin dab is effective, save and inexpensive for refractory bleeding and can be considered as the first line treatment