
Metastatic Atypical Fibroxanthoma: A Case Report
Detailed case report of an 88-year-old male with metastatic atypical fibroxanthoma skin neoplasm, including diagnosis, treatment, and outcomes. Atypical fibroxanthoma is a rare mesenchymal tumor with potential for malignancy.

Metastatic Atypical Fibroxanthoma: A Case Report
E N D
Presentation Transcript
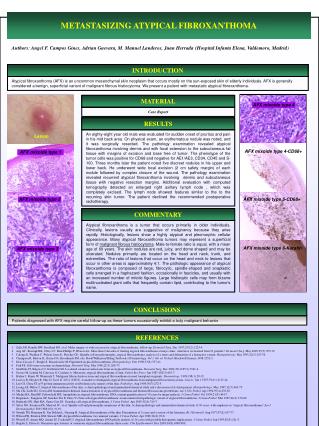
METASTASIZING ATYPICAL FIBROXANTHOMA Authors: Angel F. Campos Gines, Adrian Guevara, M. Manuel Landeros, Juan Herrada(Hospital Infanta Elena, Valdemoro, Madrid) INTRODUCTION Atypical fibroxanthoma (AFX) is an uncommon mesenchymal skin neoplasm that occurs mostly on the sun-exposed skin of elderly individuals. AFX is generally considered a benign, superficial variant of malignant fibrous histiocytoma. We present a patient with metastatic atypical fibroxanthoma. 1 2 MATERIAL AFX mixoide type 4 Case Report RESULTS An eighty-eight year old male was evaluated for sudden onset of pruritus and pain in his mid back area. On physical exam, an erythematous nodule was noted, and it was surgically resected. The pathology examination revealed atypical fibroxanthoma involving dermis and with focal extension to the subcutaneous fat tissue with margins of excision and base free of tumor. The phenotype of the tumor cells was positive for CD68 and negative for AE1/AE3, CD34, CD45 and S-100. Three months later the patient noted five discreet nodules in his upper and lower back. He underwent wide local excision (2 cm safety margin) of each nodule followed by complex closure of the wound. The pathology examination revealed recurrent atypical fibroxanthoma involving dermis and subcutaneous tissue with negative resection margins. Additional evaluation with computed tomography detected an enlarged right axillary lymph node , which was completely excised. The lymph node showed features similar to the to the recurring skin tumor. The patient declined the recommended postoperative radiotherapy. Lesion AFX mixoide type 4-CD68+ AFX mixoide type 1 AFX mixoide type 2 AFX mixoide type 5-CD68+ COMMENTARY Atypical fibroxanthoma is a tumor that occurs primarily in older individuals. Clinically, lesions usually are suggestive of malignancy because they arise rapidly. Histologically, lesions show a highly atypical and pleomorphic cellular appearance. Many atypical fibroxanthoma tumors may represent a superficial form of malignant fibrous histiocytoma. Male-to-female ratio is equal, with a mean age of 69 years. The skin nodules are red, juicy, and dome shaped and may be ulcerated. Nodules primarily are located on the head and neck, trunk, and extremities. The ratio of lesions that occur on the head and neck to lesions that occur in other areas is approximately 4:1. The pathologic appearance of atypical fibroxanthoma is composed of large, fibrocytic, spindle-shaped and anaplastic cells arranged in a haphazard fashion, occasionally in fascicles, and usually with an increased number of mitotic figures. Large histiocytic cells may form bizarre multinucleated giant cells that frequently contain lipid, contributing to the tumor's name. AFX mixoide type 6-Keratin AFX mixoide type 3 CONCLUSIONS Patients diagnosed with AFX require careful follow-up as these tumors occasionally exhibit a truly malignant behavior REFERENCES Zalla MJ, Randle HW, Brodland DG, et al. Mohs surgery vs wide excision for atypical fibroxanthoma: follow-up. Dermatol Surg. Dec 1997;23(12):1223-4. Ang GC, Roenigk RK, Otley CC, Kim Phillips P, Weaver AL. More than 2 decades of treating atypical fibroxanthoma at mayo clinic: what have we learned from 91 patients?. Dermatol Surg. May 2009;35(5):765-72. Calonje E, Wadden C, Wilson-Jones E, Fletcher CD. Spindle-cell non-pleomorphic atypical fibroxanthoma: analysis of a series and delineation of a distinctive variant. Histopathology. Mar 1993;22(3):247-54. Champion R, Burton JL, Burns DA, Breathnach SM, eds. Rook/Wilkinson/Ebling Textbook of Dermatology. Vol 3. 6th ed. Oxford: Blackwell Science;1998:2352-3. Diaz-Cascajo C, Borghi S, Bonczkowitz M. Pigmented atypical fibroxanthoma. Histopathology. Dec 1998;33(6):537-41. Fish FS. Soft tissue sarcomas in dermatology. Dermatol Surg. Mar 1996;22(3):268-73. Giuffrida TJ, Kligora CJ, Goldstein GD. Localized cutaneous metastases from an atypical fibroxanthoma. Dermatol Surg. Dec 2004;30(12 Pt 2):1561-4. Grosso M, Lentini M, Carrozza G, Catalano A. Metastatic atypical fibroxanthoma of skin. Pathol Res Pract. Jun 1987;182(3):443-7. Hafner J, Kunzi W, Weinreich T. Malignant fibrous histiocytoma and atypical fibroxanthoma in renal transplant recipients. Dermatology. 1999;198(1):29-32. Lazova R, Moynes R, May D, Scott G. LN-2 (CD74). A marker to distinguish atypical fibroxanthoma from malignant fibrous histiocytoma. Cancer. Jun 1 1997;79(11):2115-24. Lee CS, Chou ST. p53 protein immunoreactivity in fibrohistiocytic tumors of the skin. Pathology. Aug 1998;30(3):272-5. Leong AS, Milios J. Atypical fibroxanthoma of the skin: a clinicopathological and immunohistochemical study and a discussion of its histogenesis. Histopathology. May 1987;11(5):463-75. Ma CK, Zarbo RJ, Gown AM. Immunohistochemical characterization of atypical fibroxanthoma and dermatofibrosarcoma protuberans. Am J Clin Pathol. Apr 1992;97(4):478-83. Michie BA, Reid RP, Fallowfield ME. Aneuploidy in atypical fibroxanthoma: DNA content quantification of 10 cases by image analysis. J Cutan Pathol. Oct 1994;21(5):404-7. Requena L, Sangueza OP, Sanchez Yus E, Furio V. Clear-cell atypical fibroxanthoma: an uncommon histopathologic variant of atypical fibroxanthoma. J Cutan Pathol. Mar 1997;24(3):176-82. Rudisaile SN, Hurt MA, Santa Cruz DJ. Granular cell atypical fibroxanthoma. J Cutan Pathol. Apr 2005;32(4):314-7. Silvis NG, Swanson PE, Manivel JC, et al. Spindle-cell and pleomorphic neoplasms of the skin. A clinicopathologic and immunohistochemical study of 30 cases, with emphasis on "atypical fibroxanthomas".Am J Dermatopathol. Feb 1988;10(1):9-19. Starink TH, Hausman R, Van Delden L, Neering H. Atypical fibroxanthoma of the skin. Presentation of 5 cases and a review of the literature. Br J Dermatol. Aug 1977;97(2):167-77. Wilson PR, Strutton GM, Stewart MR. Atypical fibroxanthoma: two unusual variants. J Cutan Pathol. Apr 1989;16(2):93-8. Worrell JT, Ansari MQ, Ansari SJ, Cockerell CJ. Atypical fibroxanthoma: DNA ploidy analysis of 14 cases with possible histogenetic implications. J Cutan Pathol. Jun 1993;20(3):211-5. Bugatti L, Filosa G. Dermatoscopic features of cutaneous atypical fibroxanthoma: three cases. Clin Exp Dermatol. Dec 2009;34(8):e898-900.





















