Download
1 / 11
130 likes | 308 Views
Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. Authors: Tony S. Mok M.D. et al Reviewed by: Dr. Charles Butts Date posted: May 31, 2010. Thank you for downloading this update. Please feel free to use it for educational purposes.

E N D
Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma Authors: Tony S. Mok M.D. et al Reviewed by: Dr. Charles Butts Date posted: May 31, 2010
Thank you for downloading this update. Please feel free to use it for educational purposes. Please acknowledge OncologyEducation.ca and Dr. Butts when using these slides.
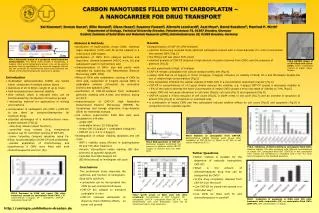
Study Design Treatment A: Gefitinib 250 mg po daily until progression R Treatment B: Carboplatin AUC 5 or 6 and Paclitaxel 200 mg/m2 i.v q21 days to max 6 cycles Stage IIIb/IV NSCLC Adenoca Non-smoker or Former Light Smoker No Prior Systemic Rx
STUDY COMMENTARY • This randomized phase III study of first line chemotherapy versus EGFR TKI was done in Asian countries • Patients selected for factors predicting presence of EGFR mutation • Overall 36% of patients had tissue evaluated for mutation status and 60% were EGFR mutation positive • Survival curves for overall population suggested two distinct populations. • Patients with EGFR mutations had higher likelihood of response and significantly longer PFS with gefitinib. • Patients lacking EGFR mutations rarely responded to gefitinib (RR1%) and were almost 3 times more likely to progress on gefitinib HR 2.85)
BOTTOM LINE FOR CANADIAN MEDICAL ONCOLOGISTS • Even in patients with clinical features that would predict for presence of EGFR activating mutations, unless actual mutation status is known, those patients would be best treated with chemotherapy. • Determination of EGFR mutation status prior to initial treatment of patients with advanced adenocarcinoma of the lung should be a priority. • For patients lacking adequate tissue for analysis, repeat biopsy if feasible should be considered. • For patients needing to be treated quickly i.e. before EGFR mutation status can be determined, chemo is a better initial option than EGFR TKI.