Download
1 / 35
360 likes | 750 Views
The Incidence of Recurrent Laryngeal Nerve Damage Following an Anterior Cervical Spine Operation. By: Brian Purcell, BSN, SRNA UPMC Hamot Medical Center School of Anesthesia/Gannon University. Recurrent Laryngeal Nerve. Recurrent Laryngeal Nerve.

E N D
The Incidence of Recurrent Laryngeal Nerve Damage Following an Anterior Cervical Spine Operation By: Brian Purcell, BSN, SRNA UPMC Hamot Medical Center School of Anesthesia/Gannon University
Recurrent Laryngeal Nerve • Branch of the Vagus Nerve, Crainial Nerve X. • Left recurrent laryngeal nerve passes at aortic arch. • Provides sensory innervation to infraglottis (Trachea below the vocal cords) • Provides motor innervation to all of the larynx except the cricothyroid muscle
Recurrent Laryngeal Nerve • Innervates all of the 1st set of Intrinsic Larynx Muscles. These muscles alter the size and shape of the larynx. • Aryepiglottic- Pulls epiglottis down over larynx • Thyroepiglottic- Assists pulling epiglottis down • Oblique arytenoid- Pulls arytenoids together
Recurrent Laryngeal Nerve • Innervates all of the 2nd set of intrinsic laryngeal muscles except the cricothyroid(External Superior Laryngeal Nerve) • These muscles move the true vocal folds • Thyroarytenoid- relaxes vocal cords • Lateral Cricoarytenoid- adducts vocal cords • Posterior Cricoarytenoid- abducts vocal cords • Traverse Arytenoid- adducts vocal cords • Vocalis- weak abduction of vocal cords
Recurrent Laryngeal Nerve • Stimulation of Recurrent Laryngeal Nerve causes abduction, opening of the vocal cords.
Recurrent Laryngeal Nerve • Damage to Recurrent Laryngeal Nerve causes vocal cord adduction, closing.
Recurrent Laryngeal Nerve • Partial damage to Recurrent Laryngeal nerve on one side will cause the cord on the same side to shut, resulting in a deterioration of voice quality • Unilateral damage usually does not compromise airway function, but airway protection against aspiration may be compromised.
Recurrent Laryngeal Nerve • Bilateral damage to Recurrent Laryngeal Nerve will cause both vocal cords to shut. This results in stridor and respiratory distress. • If the recurrent laryngeal nerve is completely severed, the vocal cords will partially close and will not move.
Recurrent Laryngeal Nerve • Symptoms of Recurrent Laryngeal Nerve damage • Unilateral: Hoarseness • Bilateral acute: Stridor, respiratory distress • Bilateral chronic: Aphonia
Damage to Recurrent Laryngeal Nerve • What can cause damage to the Recurrent Laryngeal Nerve? • Laryngoscopy • Intubation • LMA • Lesions • Trauma • Surgical Procedures
Examples of Surgical Procedures that can Cause Damage to Recurrent Laryngeal Nerve • ENT • THYROID • PARATHYROID • TRACHEAL RESECTION • NECK DISSECTION
Examples of Surgical Procedures that can Cause Damage to Recurrent Laryngeal Nerve • Thoracic • Lobectomy • Pneumonectomy • Lung Resection • Mediastinoscopy
Examples of Surgical Procedures that can Damage Recurrent Laryngeal Nerve • Vascular Surgery • Carotid Endartectomy
Examples of Surgical Procedures that can Cause Damage to Recurrent Laryngeal Nerve • General Surgery • Esophagostomy/Esophagectomy • Esophageal Diverticulectomy
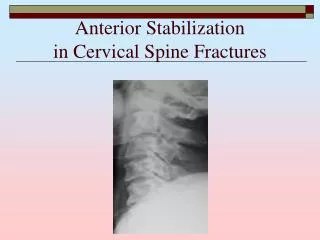
Examples of Surgical Procedures that can Cause Damage to Recurrent Laryngeal Nerve • Neurosurgery • Anterior Cervical Fusion • Involves anterior neck dissection and retraction of the soft tissue that gives exposure to the anterior vertebral column.
Anterior Cervical Spine Surgery and Recurrent Laryngeal Nerve Damage • Retraction Injury • For this surgery, Jaffe and Samuels report a 5% incidence. • The exact cause recurrent laryngeal nerve injury is not known, but it is hypothesized that compression of the recurrent laryngeal nerve within the endolarynxleads to injury(Apfelbaum, Kriskovich& Haller, 2000)
Anterior Cervical Spine Surgery and Recurrent Laryngeal Nerve Damage • What can be done to decrease or prevent the incidence? • Manipulate ETT cuff after retractor placement • Use the least amount of air possible in the ETT cuff to maintain a seal • Side of surgical approach • Replace Retractors • Monitor Recurrent laryngeal nerve during surgery
Manipulate ETT cuff after retractor insertion • Apfelbaum, Kriskovich & Hallerin 2000 studied the relationship between deflating cuff after retractor placement and re-inflating after 5 seconds. Allows ET tube to re-center within the larynx • The rate of temporary paralysis decreased from 6.4% to 1.69% using the described maneuver
Manipulate ETT cuff after retractor insertion • Audu, et al. in 2006 did not find statistical significance in their study as to the use of the above described method. • Some surgeons use the method some do not
Use just the amount of air required to create a seal in the Endotracheal tube cuff • Audu, et al describe this method as the “just seal” method. • the ETT was insufflated using the “just seal” method as follows: With the ETT cuff deflated, positive pressure (20–25 cm H2O) was generated in the breathing circuit while listening for an air leak around the ETT. The cuff was then insufflated with air until the leak was obliterated.
Use just the amount of air required to create a seal in the Endotracheal tube cuff • Audu et al in 2006 did not find statistical significance in decreasing incidence of vocal cord paralysis associated with recurrent laryngeal nerve damage • Jung and Schramm published in 2010 did find significance in in decreased incidence of paralysis with lower ETT cuff pressures
Side of surgical approach • Jung and Schramm (2010) report that in conjunction with maintaining low ETT cuff pressures, the left side approach reduced the incidence of vocal cord paralysis
Replace Retractors • Rackesh et al. (2010) conducted a study that found cuff pressure in general may be the cause of vocal cord paralysis. • Conclusions were to create a “just seal” and possibly institute intermittent release of the retractors which would keep the cuff pressures at an acceptable level
Monitor Recurrent Laryngeal Nerve Intra-operatively • Tisdall, M., Henn, C., & Dorward, N. (2010) study on 19 patients using vagal/recurrent laryngeal nerve stimulation to monitor the integrity of the recurrent laryngeal nerve. • With small sample size, researchers concluded that intraoperative monitoring may potentially reduce the incidence of recurrent laryngeal nerve palsy.
Monitor Recurrent Laryngeal Nerve Intra-operatively • Stimulation monitoring similar to that used in Thyroid surgery, where such monitoring is manditory • Monitoring identifies the recurrent laryngeal nerve, and can identify areas of concern which can be avoided to reduce recurrent laryngeal nerve injury • Tisdall, M., Henn, C., & Dorward, N. (2010)
Conclusions • Recurrent Laryngeal Nerve is Branch of Cranial Nerve X (Vagus Nerve) • Left recurrent laryngeal nerve passes at the aortic arch • Provides sensory innervation to infraglottis (Trachea below the vocal cords) • Provides motor innervation to all of the larynx except the cricothyroid muscle
Conclusions • Stimulation of Recurrent Laryngeal Nerve causes abduction, opening of the vocal cords. • Damage to Recurrent Laryngeal Nerve causes vocal cord adduction, closing. • Unilateral damage causes vocal cord on same side as the damage to close. This can result in hoarseness and the inability to protect against aspiration.
Conclusions • Bilateral damage will cause both cords to close and will result in respiratory distress • Damage to recurrent laryngeal nerve during anterior cervical surgery is thought to be caused by compression of the caused by retractor placement. • Recurrent laryngeal nerve damage is the most common ENT complication associated with anterior cervical procedures.
Conclusions • Methods of preventing recurrent laryngeal nerve injury: • Manipulate the endotracheal tube cuff after retractor placement. • Create a “just seal” with ETT cuff • Possibly perform surgery from left side. • Stimulation monitoring of recurrent laryngeal nerve
Conclusions • Still no concrete standard of care in preventing recurrent laryngeal nerve damage. • More study and research needs to be completed to create a concrete standard of care.
References • Apfelbaum, R., Kriskovich, M., & Haller, J. (2000). On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine, 25(22), 2906-2912. • Audu, P., Artz, G., Scheid, S., Harrop, J., Albert, T., Vaccaro, A., & ... Rosen, M. (2006). Recurrent laryngeal nerve palsy after anterior cervical spine surgery: the impact of endotracheal tube cuff deflation, reinflation, and pressure adjustment. Anesthesiology, 105(5), 898-901.
References • Jaffe, R., & Samuels, S. (2009). Anesthesiologist's manual of surgical procedures. (4th ed.). Philadelphia: Lippincott, Williams & Wilkins, a Wolters Kluwer business. • Jung, A., & Schramm, J. (2010). How to Reduce Recurrent Laryngeal Nerve Palsy in Anterior Cervical Spine Surgery: A Prospective Observational Study. Neurosurgery (67)1, 10-15
References • Rakesh, G., Girija,R., Parmod, B., Hemansh, P., Manish, M. (2010). Clinical Investigation Effects of Retractor Application on Cuff Pressure and Vocal Cord Function in Patients Undergoing Anterior Cervical Discectomy and Fusion. Indian Journal of Anaesthesia (54)4, 292-295. DOI: 10.4103/0019-5049.68370 • Tisdall, M., Henn, C., & Dorward, N. (2010). Intra-operative Recurrent Laryngeal Nerve Stimulation During Anterior Cervical Discectomy: A Simple and Effective Technique. British Journal of Neurosurgery (24)1, 77-79. DOI: 10.3109/02688690903398459