Download
1 / 16
170 likes | 505 Views
LymphoStat-B TM A Case Study for Endpoints and Trial Design in SLE. Presentation to the Arthritis Drugs Advisory Committee 30 September 2003 Bill Freimuth, MD, PhD. Agenda. Review BLyS and the pharmacologic rationale, nonclinical and clinical data for LymphoStat-B

E N D
LymphoStat-BTMA Case Study for Endpoints and Trial Design in SLE Presentation to the Arthritis Drugs Advisory Committee30 September 2003 Bill Freimuth, MD, PhD
Agenda • Review BLyS and the pharmacologic rationale, nonclinical and clinical data for LymphoStat-B • Review phase 2 trial design in SLE • Pose questions related to SLE trial design/endpoints to the Committee for discussion
BLyS • B-Lymphocyte Stimulator • Identified in a high-throughput proliferation assay • A member of the TNF family • Alternate names: • TALL-1, zTNF4, THANK, BAFF & TNFSF-20 • Biologically active, soluble form is a 51 kd homotrimer • Binds 3 membrane receptors on B lymphocytes • Acts as a survival factor by inhibiting B-cell apoptosis • Stimulates differentiation of B cells to Ig-producing plasma cells
Rationale for BLyS Antagonists in SLE • Mouse data links BLyS and autoimmune disease • Transgenic models over-expressing BLyS have autoimmune/SLE-like phenotype • Genetic models of autoimmune disease have elevated levels of circulating BLyS • Soluble BLyS receptors administered in an animal model of SLE ameliorates disease progression and improves survival • Elevated BLyS levels are evident in the serum of SLE and RA patients • BLyS levels positively correlated with serum IgG and autoantibody levels
Autoimmune Patients Display Elevated Serum BLyS Concentrations 5 0 Normal vs SLE or RA, p <0.001 4 0 3 0 BLyS concentration (ng/mL) 2 0 1 0 0 Normal SLE1 SLE2 RA RAsf (From Zhang et al, J Immunol, 2001)
LymphoStat-B Inhibits BLyS Effects in Mice • Human BLyS administration stimulates increased spleen weight, B220+/ThB+ splenic B cell numbers and serum IgA • LymphoStat-B is a fully human IgG1l monoclonal antibody that specifically recognizes and binds to soluble human BLyS • LymphoStat-B selectively inhibits these BLyS-induced effects
LymphoStat-B Inhibits BLyS Induced Serum IgA Increase # 700 # p <0.05 600 # 500 400 Serum IgA (g/mL) # # # # 300 200 100 0 5.0 0.05 0.15 0.5 1.5 5.0 0.05 0.15 0.5 1.5 Naive LymphoStat-B(mg/kg) IgG1 control(mg/kg) Ab Buffer + BLyS Ab Buffer + BLyS Buffer
LymphoStat-B: Activity and Safety in Cynomolgus Monkeys • LymphoStat-B was well tolerated at doses up to 50 mg/kg q2 weeks for 6 months and during an 8-month recovery period • No study agent-related infections during treatment or recovery periods • Activity of LymphoStat-B is demonstrated by decreases in B lymphocytes • Flow cytometry, organ weights and histologic findings correlated with effects on B lymphocytes • PK are linear, with a terminal half-life of ~11-14 days • Complete results to be presented at ACR
LymphoStat-B Reduces CD20+ Peripheral Blood B-lymphocytes * Statistically significant difference from vehicle control 250 0 mg/kg/dose 5 mg/kg/dose 225 15 mg/kg/dose 200 50 mg/kg/dose 175 150 99% % Baseline CD20+ Cells 125 100 41% 42% 75 * * * 35% * * * * * 50 * * * * 25 0 Week 13 Week 26 Week 33 Week 39 Week 45 Week 52 Week 60 Treatment Recovery Animals per dose group: 12/16 8/10 4 4 4 4 4
LymphoStat-B: Clinical Development in SLE • Phase 1 Clinical Trial • 4 IV doses (1, 4, 10 and 20 mg/kg) and placebo evaluated as a single dose or 2 doses 21 days apart • Well tolerated • No drug-related serious adverse events • No increase in adverse events or laboratory abnormalities • No increase in incidence of infection • Linear pharmacokinetics with ~14 day half-life • Biological activity observed • Complete results to be presented at ACR • Fast Track Designation granted
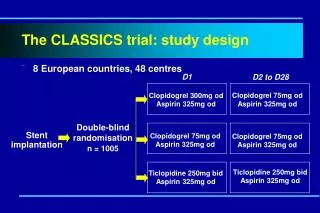
LymphoStat-B: Phase 2 SLE Trial Design • Multi-center, randomized, double-blind, placebo-controlled, dose-ranging (1, 4, 10 mg/kg) • Patients with active SLE (SELENA SLEDAI > 4) and on stable medications • 350 patients • IV administration Day 0, 14, 28 then q28 days for 1 year
LymphoStat-B: Phase 2 SLE Trial Design • Primary endpoints • SELENA SLEDAI activity at week 24 • Time to first flare (defined by SELENA SLEDAI flare index) over 52 weeks • Sample Size • 80% power, 0.05, to detect in 1 of the active groups • a 25% absolute or 100% relative improvement (e.g., 25% to 50%) in the percent change from baseline score in SELENA SLEDAI at Week 24 and • a reduction in the percent of subjects having their first flare by Week 52 from 65% to 43%
LymphoStat-B: Phase 2 SLE Trial Design • Major secondary endpoints • Week 52 SELENA SLEDAI and BILAG scores • Time to first flare (defined by BILAG) over 52 weeks • Reduction in steroid use • AUC of SELENA SLEDAI and BILAG over 52 weeks • Biological markers • Anti-dsDNA, ANA, and C3 and C4 levels • B cells (CD20+, CD27+, CD69+) and plasmacytoid cells (CD138+, CD19/CD27BRIGHT) • Total serum IgG and other subclasses
Questions for Committee Discussion • Would an effect in either SELENA SLEDAI at 24 weeks or time to first flare over 52 weeks be an adequate basis to move forward to a confirmatory trial? • Which endpoint is thought to be more clinically meaningful? • Is the magnitude of effect being tested for clinically relevant? Would a lesser effect also be clinically meaningful?
Questions for Committee Discussion • Are there other endpoints that would be preferred and considered more clinically meaningful? For example: • Would significant benefit in one or more specific SLE organ system manifestations (as defined in BILAG) be a relevant primary endpoint? • Would a significant steroid-sparing effect with or without a positive trend in disease activity and/or flare be a sufficient primary endpoint? • Which endpoint would be the most compelling as a primary endpoint in a pivotal trial?
Questions for Committee Discussion • Several other clinical endpoints and markers of biological activity are being explored • Which are believed to be the more meaningful? • Is there currently sufficient evidence to consider any of these biomarkers reasonably likely to predict clinical benefit?