Radiological Findings and Diagnoses: Insights and Interpretations
Study of various radiographic findings including empty sella syndrome, dental cyst, anomalous pulmonary artery, toxoplasmosis, and more. Detailed interpretations and diagnosis in known cases discussed.


Radiological Findings and Diagnoses: Insights and Interpretations
E N D
Presentation Transcript
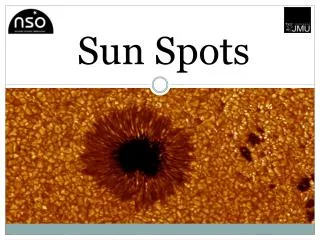
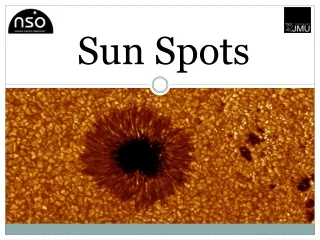
SPOTS BHUMIKA SUTHAR THIRD YEAR RESIDENT SSGH,BARODA 03/10/08
EMTY SELLA SYNDROME The CT scan shows symmetrical cranial contents. The pituitary fossa shows low density with no enhancement in these cuts, after intravenous contrast. The MRI confirms the lack of soft tissue in the fossa. There is a posterior line of soft tissue, which may represent the functioning hypophysis.
Dental cyst dental CT, which showed a well-defined, odontogenic lesion, with its epicentre in relation to the root of the first molar tooth, but extending from the second premolar to the second molar . This appearance is highly suggestive of a dental cyst, also called a radicular or apical or periapical cyst. It occurs as a result of root infection.
Anomalous origin of the left pulmonary artery from right Posteroanterior chest radiograph shows an anomalous right paratracheal border (arrowheads). Unenhanced CT scan and MR angiogram at the level of the pulmonary trunk show the abnormal course of the left pulmonary artery (arrowheads in b) between the lower portion of the trachea and the esophagus
The anomalous pulmonary artery may be accompanied by tracheobronchial stenosis resulting from complete cartilaginous RINGS------ a life threatening feature in infants called the RING-SLING COMPLEX.
TOXOPLASMOSIS There are scattered spots of amorphous calcific density. Some form a line that corresponds to the location of the lateral ventricles. The unfused sutures are not widened and the dosum sellae is intact. There is no calcification in the orbit.
NORMAL DIPLOIC LAKES well-defined lytic areas in the skull vault, often with visible diploic vessels going to them. Their location is intradiploic. There is no vault expansion. The inner and outer tables are intact.
This radiographic compression view of the kidneys was obtained at 15 minutes after the intravenous injection of contrast material and shows linear striations of contrast material that opacify the collecting tubules, giving a paintbrush-like appearance that is typical of medullary sponge kidney.
7. A three-phase bone scan Blood flow Blood pool Delayed
demonstrate focal hyperperfusion, focal increased activity, and intense focal uptake, in the right great toe in a case of osteomyelitis. It can be differentiated from the cellulitis ,where abnormal increase in activity is seen on blood flow and blood pool phase but not on delayed images. The pattern of abnormal persistent uptakeat 24hrs is consistent with the diagnosis ofosteomyelitis.
TUBERCULOUS DACTILYTIS(SPINA VENTOSA) TRANSPHYSEAL SPREAD, NO ARTHRITIS As underlying bone is destroyed, a cyst-like cavity forms and the remaining bone appears to be ballooned out. This appearance is termed spina ventosa ("wind-filled sail").
primary sclerosing cholangitis. shows intrahepatic and extrahepatic bile duct strictures and irregularities.
10. Give diagnosis…in known case of HIV POST Gd T1W T2W IMAGE
LYMPHOEPITHELIAL CYSTS Enhanced fat saturation and T2W MR images demonstrate multiple cysts (arrowheads) within the parotid glands. The lesions are hypointense on T1-weighted and hyperintense on T2-weighted images.
Osteochondroma (a) Axial CECT scan at the level of the left atrium (A) shows a dense calcification (arrowhead) that projects medially from a right rib
REVERSAL SIGN Transverse unenhanced CT scans demonstrate reversal sign with decreased attenuation overall and loss of gray-white differentiation. Note relatively increased attenuation of (a) basal ganglia (arrows), (b) thalami (thin arrows), and cerebellum (wide arrows).
The reversal sign indicates diffuse cerebral injury in a patient who has suffered an anoxic insult. Causes of the reversal sign include head trauma, hypoxia, birth asphyxia, drowning, status epilepticus, hypothermia, bacterial meningitis, strangulation, nonaccidental trauma, and other causes of global cerebral ischemia Pathogenesis of the reversal sign is complex and not yet fully understood. One theory is that preservation of central structures is due to transtentorial herniation secondary to acute edema, with pressure partially relieved as the brain herniates through the incisura. The pressure relief is thought to improve tissue perfusion to central structures, thus delaying or preventing necrosis.
The relative preservation of attenuation in the posterior fossa likely reflects preferential maintenance of blood flow in the posterior circulation relative to that in the anterior circulation. Other researchers have suggested that postischemic hypervascularity may cause the relatively increased attenuation seen in the thalami and basal ganglia. However, administration of intravenous contrast material does not aid in the detection of the reversal sign The reversal sign is associated with a poor prognosis and indicates irreversible brain damage.
Pneumatosis cystoides coli. Appear polyposis-like from an endoluminal image, On 2D images, the air composition of these cysts is readily apparent. Pneumatosis cystoides coli. (a) Endoluminal 3D view from CTC shows multiple polypoid lesions. some lesions are "shelled out" and appear more like diverticula(b) Axial 2D image shows that lesions all represent thin-walled, air-filled cysts. Localized subserosal dissection of air surrounds this bowel loop, but no free intraperitoneal air
Finding Transverse CT scan with oral and intravenous contrast material demonstrates dependent viscera sign on the left side of a 32-year-old man. The stomach (arrow), which contains food and oral contrast material, abuts the posterior ribs on the left side and is posterior to the top of the spleen (arrowhead).
EXPLANATION The dependent viscera sign is seen with diaphragmatic rupture. The absence of posterior support by the diaphragm allows viscera to "fall" against the posterior ribs to a dependent position. On the right side, the upper one-third of the liver typically does not abut the posterior chest wall (ie, the right ribs) when the diaphragm is intact. On the left side, the stomach and bowel lie anterior to the spleen and generally do not abut the left ribs when the diaphragm is intact. Therefore, the dependent viscera sign is said to be present on the right side if the upper one-third of the liver abuts the posterior ribs and on the left side if the stomach or bowel abuts the posterior ribs or lies posterior to the spleen. The most common site of diaphragmatic rupture is at the posterior-lateral aspect of the pleuroperitoneal membrane Imaging studies suggest a predominance of left-sided injury, with postmortem studies indicating an equal distribution
15 T1
A Chiari I malformation involves caudal displacement of the Cerebellar tonsils below the foramen magnum (tonsilar ectopia). Here vermis, fourth ventricle, medulla are usually normal or minimally displaced. Associated brain anomalies are not seen. Myelomeningocele is a not a feature of Chiari I malformation.
Syrinx is present in 30-60% of all patient with the Chiari I and 60-90 % in symptomatic patient. Cervical spinal cord is the common site. Mild to moderate hydrocephalus (20-25%) Normally positioned fourth ventricle. Age-criteria for tonsilar ectopia are: 6mm – 1-10 yrs 5mm _ 10-30 yrs 4mm _ 30-80 yrs 3mm _ >80 yrs
Diagnosis Superior Mesenteric Artery Syndrome
Medulloblastoma is generally thought to be a type of primitive neuroectodermal tumor (PNET) which has differentiated along neuronal lines. Over 90% of medulloblastomas are midline arising in the cerebellar vermis along the roof of the fourth ventricle in young children. Most patients (75%) are less than 15 years of age, with half being less than 10 years old. More males are affected than females. There is a small, second peak in young adults, aged 24-30 years. In these patients and in adolescents, the tumors are more likely to be centered in one of the cerebellar hemispheres. The midline tumors grow anteriorly into the fourth ventricle and posteriorly through the foramen of Magendie into the cisterna magna. Therefore, the tumors often present with signs of obstructive hydrocephalus including headache, nausea, and vomiting. Visual and motor disturbances are also common.
The "typical" medulloblastoma has characteristic findings. On CT, the midline mass is slightly hyperdense to normal cortex before contrast, and demonstrates diffuse, intense, homogeneous enhancement following contrast administration. Calcification and gross cystic spaces are rare. On MR, the mass is heterogeneously hypo- to isointense to normal cortex on T1-weighted images, hypo- to hyperintense on T2-weighted images, and enhances moderately intensely after gadolinium administration. Medulloblastoma spreads along the CSF pathways leading to the development of suprasellar masses, masses on the surface of the brain, ependymal implants along the ventricular surfaces, and "drop metastases" along the spinal cord. Parenchymal masses can also occur due to spread along the Virchow-Robin spaces. All patients should be evaluated for the presence of CNS metastatic disease. Gadolinium-enhanced MR of the brain and spine has the best resolution, although CSF flow and respiratory movement may limit its sensitivity. Metastases also occur to bone, though less commonly, creating lytic and sometimes blastic lesions.
18 Post Gd fat sat.axial T1W
optic nerve tram-track sign in c/o optic nerve sheath Meningiomas
The optic nerve tram-track sign is most commonly described in relation to optic nerve sheath Meningiomas. Meningiomas tend to cause segmental or diffuse circumferential thickening of the optic nerve sheath. Once intravenous contrast material has been administered, the optic nerve can be seen on CT or MR images as an unenhanced central linear structure (negative defect) surrounded by the enhanced Meningioma. On transverse or Sagittal images this produces a tram-track sign, which is composed of two enhanced areas of tumor separated from each other by the negative defect of the optic nerve. The corresponding finding on coronal images is a doughnut configuration. Though it is less common, the tram-track sign may be evident at unenhanced CT when there is linear calcification of the optic nerve sheath Meningioma.
CONTINUOUS DIAPHRAGM SIGN Pneumomediastinum