Download
1 / 96
970 likes | 1.19k Views
Role of Anticoagulants in ACS. Bashir Hanif , MD, FACC, FSCAI Medical Director Chief of Cardiology Tabba Heart Institute. Overview. Brief Epidemiology and Pathophysiology Overview of Anticoagulants used in ACS Is there Evidence What the Guidelines say? Innovative Ideas from South Korea.

E N D
Role of Anticoagulants in ACS BashirHanif, MD, FACC, FSCAI Medical Director Chief of Cardiology Tabba Heart Institute
Overview • Brief Epidemiology and Pathophysiology • Overview of Anticoagulants used in ACS • Is there Evidence • What the Guidelines say? • Innovative Ideas from South Korea
Epidemiology of ACS in the United States • Single largest cause of death • 515,204 US deaths in 2000 • 1 in every 5 US deaths • Incidence • 1,100,000 Americans will have a new or recurrent coronary attack each year and about 45% will die* • 550,000 new cases of angina per year • Prevalence • 12,900,000 with a history of MI, angina, or both * Based on data from the ARIC study of the National Heart, Lung, and Blood Institute, 1987-1994. Includes Americans hospitalized with definite or probable MI or fatal CHD, not including silent MIs. ACS indicates acute coronary syndrome; MI, myocardial infarction; ARIC, Atherosclerotic Risk in Communities; and CHD, coronary heart disease. From American Heart Association. Heart Disease and Stroke Statistics—2003 Update.
Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57 Million Hospital Admissions - ACS UA/NSTEMI† STEMI 1.24 millionAdmissions per year 0.33 millionAdmissions per year *Primary and secondary diagnoses. †About 0.57 million NSTEMI and 0.67 million UA. Heart Disease and Stroke Statistics – 2007 Update. Circulation 2007; 115:69–171.
Causes of UA/NSTEMI* • Thrombus or thromboembolism, usually arising on disrupted or eroded plaque • Occlusive thrombus, usually with collateral vessels† • Subtotally occlusive thrombus on pre-existing plaque • Distal microvascular thromboembolism from plaque-associated thrombus • Thromboembolism from plaque erosion • Non–plaque-associated coronary thromboembolism • Dynamic obstruction (coronary spasm‡ or vascoconstriction) of epicardial and/or microvascular vessels • Progressive mechanical obstruction to coronary flow • Coronary arterial inflammation • Secondary UA • Coronary artery dissection§ *These causes are not mutually exclusive; some patients have 2 or more causes. †DeWood MA, et al. N Engl J Med 1986;315:417–23. ‡May occur on top of an atherosclerotic plaque, producing missed-etiology angina or UA/NSTEMI. §Rare. Modified with permission from Braunwald E. Circulation 1998;98:2219–22. Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157, Table 3.
Pathogenesis of ACS Plaque rupture Platelet adhesion Platelet activation Partially occlusive arterial thrombosis & unstable angina Microembolization & non-ST-segment elevation MI Totally occlusive arterial thrombosis & ST-segment elevation MI White HD. Am J Cardiol 1997;80 (4A):2B-10B.
Thrombus Formation and ACS Plaque Disruption/Fissure/Erosion Thrombus Formation Old Terminology: UA NQMI STE-MI New Terminology: Non-ST-Segment Elevation Acute Coronary Syndrome (ACS) ST-Segment Elevation (ACS)
Plaque Rupture Thrombus Mechanical Vasoconstrictive Serotonin Release Distal Embolization Vasoconstriction Mechanical Plugging
The Role of the Platelet in Non-ST-segment Elevation Acute Coronary Syndromes (NSTE ACS) Results from cross-linking of platelets by fibrinogen atplatelet receptors GP IIb-IIIaat site of plaque rupture Generally caused by partially-occlusive, platelet-rich thrombus in a coronary artery Unobstructedlumen GP IIb-IIIa Platelet Thrombus Fibrinogen Rupturedplaque Artery wall Van de Werf F. Throm Haemost 1997;78(1):210-213.
The Role of the Thrombus in ST-segment Elevation MI (STEMI) Generally caused by a completely occlusive thrombus in a coronary artery Results from stabilization by fibrin mesh of a platelet aggregate at site of plaque rupture platelet RBC fibrin mesh Van de Werf F. Throm Haemost 1997;78(1):210-213.
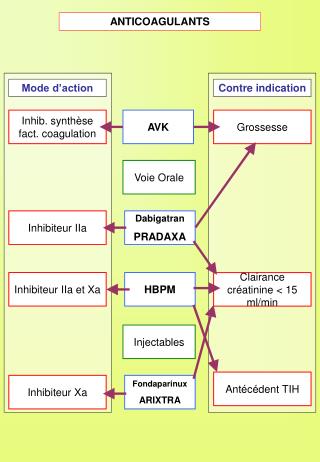
Anticoagulants • Heparins • Unfractionated heparin (UFH) • Low molecular weight heparin (LMWH) • Enoxaparin, Dalteparin • Factor X-A Inhibitor • Fondaparinux • Direct Thrombin Inhibitors • Bivalirudin: reversible binding • Lepirudin: irreversible binding • Argatroban: reversible binding • Hirudin
Anticoagulants and Gymnastics • Anticoagulation is like a • performance beam • Both efficacy and safety are • important. • If you fail to balance efficacy • and safety patient may get hurt
The Search for an Anticoagulant That Balances Safety and Efficacy Optimal Safety and Efficacy Thrombosis Bleeding Dose (concentration) of Anticoagulant
Unfractionated Heparin An unbranched heteropolysaccharide Chain
Unfractionated Heparin (UFH) • Binds antithrombin & inhibits clotting factors Xa & IIa (thrombin) • IV bolus followed by infusion, adjust according to aPTT or antifactor Xa levels • Can be used in patients with renal dysfunction
Unfractionated Heparin (UFH) • NSTE ACS • preferred anticoagulant following angiography in patients undergoing CABG (Class 1) • option for patients undergoing planned early angiography & revascularization (Class 1) • may be used in patients in whom an initial conservative strategy is planned (Class 1) • 1st line anticoagulant for STE ACS & PCI • administered with a fibrin selective fibrinolytic (Class 1)
Unfractionated Heparin (UFH) • Contraindications: • history of heparin induced thrombocytopenia (HIT) • active bleeding • severe bleeding risk • recent stroke • Adverse effects: • bleeding • HIT
Enoxaparin • Shorter chain length compared to UFH • more predictable effects • Binds antithrombin, inhibits factors Xa & IIa • Contraindications: • active bleeding, severe bleeding risk • history of HIT • recent stroke • CrCl < 15 ml/min • avoid in CABG patients • Dose: 1 mg/kg every 12 hrs (renal adjustment required) • Adverse effects: bleeding & HIT (lesser extent than UFH)
Enoxaparin • STEMI • not studied in primary PCI (Class 2b as alternative to UFH) • NSTEMI ACS • option for patients undergoing planned early angiography and revascularization (Class 2a) • UFH recommended over enoxaparin or fondaparinux (Class 1b) • may be used in patients in whom an initial conservative strategy is planned (Class 1) • fondaparinux recommended over enoxaparin (Class 1a) • enoxaparin recommended over UFH (Class 1b) Schünemann HJ, Hirsh J, Guyatt G, et al. Executive Summary: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133;71-109.
Limitations with Current Anticoagulation Therapy Albans S et al. Eur J Clin Invest 2005;35(Suppl 1):12-20.
Comparison of Heparin + ASA vs ASA Alone Theroux RISC Cohen 1990 ATACS Holdright Gurfinkel Summary Relative Risk 0.67 (0.44-0.1.02) 0.1 1 10 RR: Death/MI ASA Alone 68/655=10.4% Heparin + ASA 55/698=7.9% ASA indicates acetylsalicylic acid; RISC, Research on InStability in Coronary artery disease; ATACS, Antithrombotic Therapy in Acute Company Syndromes; RR, relative risk; and MI, myocardial infarction. Data from Oler A, Whooley MA, Oler J, et al.Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina: a meta-analysis. JAMA. 1996;276:811-815. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.
ESSENCE: Study Design (n=1607) Enoxaparin 1mg/kg q 12 H Subcutaneous + ASA Follow-up Visit Day 14 Follow-up Call Day 30 Unstable Angina Non-Q-Wave MI UFH IV dose-adjusted + ASA Follow-up Visit Day 14 Follow-up Call Day 30 (n=1564) Treatment Phase min 48 H, max 8 Days Follow-up Phase Cohen, et al. NEJM 1997;337:447-52
ESSENCEAll Randomized 30 Heparin Enoxaparin 23.3% 25 19.8% 20 19.8% % Death, MI or RA 16.6% RRR 15 % P=0.016 15 RRR 16.2 % P=0.019 10 5 0 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 Time (Days) Cohen, et al. NEJM 1997;337:447-52
ESSENCE 1 Year Data p=0.022 p=0.033 p=0.042 % Incidence of Triple Endpoint p=0.023 (n= 1564) (n=1607) Goodman SG, et al. JACC 2000;36:693-8
TIMI 11 B Study Design Enoxaparin 30 mg IV bolus + 1mg/kg SC q 12 hr Fixed Dose < 65 kg > 65 kg 40 mg 60 mg q 12 hr SC (n=1953) Unstable Angina Non-Q Wave MI 24 h ASA UFH 70 U/kg IV bolus + 15 U/kg/hr IV 72h Fixed Dose Placebo q 12 hr SC (n=1957) Acute Phase min 72H, max 8 Days Chronic Phase 43 days Antman et al, Circulation 1999;100:1593-601
1 6 . 7 % 1 4 . 2 % TIMI 11B: Enoxaparin vs. Heparin in NSTE-ACS 20 Unfractionated Heparin Enoxaparin (Lovenox) 16 12 Death, MI or Urgent Revascularization 8 p = 0.03 Relative Risk Reduction = 15% 4 0 2 4 6 8 10 12 14 Days Adapted from Antman EM, et al. Circulation. 1999;100:1593-1601.
TIMI 11B-ESSENCE Meta-AnalysisDeath/MI TIMI 11B 3910 B ESSENCE 8 3171 OVERALL 7081 5.3 4.1 0.77(0.62-0.96) 0.02 23 B TIMI 11B 3910 B 14 ESSENCE 3171 B 0.79(0.65-0.96) 21 0.02 OVERALL 7081 6.5 5.2 3910 TIMI 11B B 3171 ESSENCE 43 B 0.82(0.69-0.98) 18 0.02 OVERALL 7081 8.6 7.1 N Enox(%) Day UFH(%) OR p % 0.5 0.6 0.7 0.8 0.9 1 2 Enox Better Odds Ratio UFH Better
Enoxaparin in STEMI: ExTRACT-TIMI 25 STEMI < 6 hourslytic eligible Acetylsalicylic acid (ASA) Lytic choice by physician (TNK,TPA, rPA, SK) Double-blind double dummy phase Enoxaparin< 75 y: 30 mg IV bolus sc 1.0 mg/kg q 12h (Hosp DC)≥ 75 y: No bolus sc 0.75 mg/kg q 12h (Hosp DC) CrCl ≤ 30: 1.0 mg/kg q 24 h UFHbolus 60 U/kg infusion 12 U/kg/h for ≥ 48 hours Day 30 Primary Efficacy Endpoint: Death or non fatal MIPrimary Safety Endpoint: TIMI Major Hemorrhage STEMI: ST-segment elevation myocardial infarction;MI:Myocardialinfarction; TIMI:Thrombolysis in Myocardial Infarction TNK: Tenecteplase; TPA: Tissue plasminogen activator; rPA: Reteplase; SK: Streptokinase; UFH: Unfractionated heparin; CrCl: Creatinine clearance
ExTRACT-TIMI 25Primary endpoint: Death or non fatal MI Lost to follow up = 3 48 h 8 days 15 UFH 12.0% 12 206 events 9.3% 9.9% 9 5.2% Enoxaparin Primary Endpoint (%) 7.2% 6 4.7% RR: 0.83, (0.77–0.90) p<0.0001 RR: 0.77 (0.71– 0.85)p<0.0001 3 RR: 0.90 (0.80–1.01)p=0.08 0 0 5 10 15 20 25 30 Days *ITT: Intent-to-treat Antman EM et al. for the ExTRACT-TIMI 25 Investigators. N Engl J Med 2006;354:1477-88
Fondaparinux • Inhibits factor Xa and Thrombin • less likely to cause HIT than UFH, LMWH • STE ACS • alternative to UFH in patients not undergoing reperfusion (Class 1) or receiving fibrinolytics (Class 2b) • not recommended for use alone in 1˚ PCI (Class 1a) • Schünemann HJ, Hirsh J, Guyatt G, et al. Executive Summary: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133;71-109.
Fondaparinux • NSTE ACS • option for patients undergoing planned early angiography & revascularization with PCI • option for patients in whom an initial conservative strategy is planned • preferred agent for patients with high risk for bleeding (Class 1)