Download
1 / 38
400 likes | 682 Views
Sleep and Health. Patrick J. Strollo, Jr., M.D. University of Pittsburgh Medical Center. PMBC SLEEP WORKSHOP 2006. Goals. Review how disturbed sleep impacts physiology in healthy humans Examine the data relating disturbed sleep to morbidity and mortality

E N D
Sleep and Health Patrick J. Strollo, Jr., M.D.University of Pittsburgh Medical Center PMBC SLEEP WORKSHOP 2006
Goals • Review how disturbed sleep impacts physiology in healthyhumans • Examine the data relating disturbed sleep to morbidity and mortality • Understand how a common sleep disorder (Sleep Apnea) may the contribute to cardiovascular risk • Appreciate the complex interaction between disturbed sleep and physiologic risk in patient populations
Consolidate memory Improve concentration Improve mood Enhance creativity Hormonal control of appetite Immune function & systemic inflammation Function of Sleep Brain Systemically Sleep Medicine 2004 5:225-30 Nature 2004 430:27-28 J Am Coll Cardiol 2004 43:678-83 J Clin Endocrinol Metab 2004 89:5762-71
Interaction between Sleep and Wake States NREM WAKE REM
Effect of insufficient sleep on unadjusted prevalence rates for HRQOL among adults aged 18 or older (n = 79,625) > 14 / 30 days insufficient sleep < 14 / 30 days insufficient sleep Sleep Med 2005 6:23-27
The Cumulative Cost of Additional Wakefulness: Dose-Response Effects on Neurobehavioral Functions and Sleep Physiology From Chronic Sleep Restriction and Total Sleep Deprivation Aim: Assess whether human sleep can be chronically reduced without consequences Design: The chronic sleep restriction experiment involved randomization to 1 of 3 sleep doses (4 h, 6 h, or 8 h time in bed per night), which were maintained for 14 consecutive days. The total sleep deprivation experiment involved 3 nights without sleep (0 h time in bed). Each study also involved 3 baseline (pre-deprivation) days and 3 recovery days. Subjects: A total of n = 48 healthy adults (ages 21–38) Results: Chronic restriction of sleep periods to 4 h or 6 h per night over 14 consecutive days resulted in significant cumulative, dose-dependent deficits in cognitive performance on all tasks. Conclusion: Chronic restriction of sleep to 6 h or less per night produced cognitive performance deficits equivalent to up to 2 nights of total sleep deprivation, relatively moderate sleep restriction can seriously impair waking neurobehavioral function in healthy adults. SLEEP 2003 2:117-126
Impact of Sleep Debt on Metabolic And Endocrine Function Lancet 1999 354:1435-39 Sleepiness p < 0.0001 Stanford Sleepiness Score 1000 – 1400 h • Aim: Examine the effect of sleep debt • on metabolic and hormonal function • Subjects: 11 Males (18 -27 yrs) • Design: • Baseline - 3 nights 8 hrs in bed • Sleep Debt - 6 nights 4 hrs in bed • Recovery – 7 nights 12 hrs in bed • Results: In the Sleep Debt Condition • Glucose tolerance & thryrotropin • concentrations were decreased • Evening cortisol concentrations were • increased • Sympathetic nervous system activity • was increased Sympathovagal Balance p < 0.02 Sympathovagal Balance 0900 -1400 h Evening cortisol concentrations p < 0.007 Saliva Free Cortisol Mmol/L 1600 - 2000 h 8 12 4 Time in Bed
Sleep Curtailment in Healthy Young Men Is Associated with Decreased Leptin Levels, Elevated Ghrelin Levels, and Increased Hunger and Appetite Ann Intern Med 2004 141:846-850 After 2 d of 10-h sleep time After 2 d of 4-h sleep time After 2 d of 4-h sleep time • Aim: To determine whether partial • sleep curtailment, alters appetite • Subjects: 12 normal weight males • BMI 23.6 + 2.0 / Age 22 + 2 yrs • Design: Randomized, 2 period, • 2 condition crossover clinical study • Intervention: 2 days of sleep restriction • and 2 days of sleep extension • Results: Sleep restriction was associated • with – • Decreased Leptin (anorexigenic) 18% • Increased Ghrelin (orexigenic) 24% • Increased Hunger 24% • Increased appetite* 23% • *calorie dense high carbohydrate food After 2 d of 10-h sleep time After 2 d of 4-h sleep time After 2 d of 10-h sleep time After 2 d of 4-h sleep time After 2 d of 10-h sleep time
The association between total sleep time and body weight in primary care Results: Aim: Examine the association between restricted sleep and obesity in a heterogeneous adult primary care population Design: Prospective cohort, involving questionnaires and measurement of BMI in 4 primary care offices (n = 1001) Conclusion: Reduced amounts of sleep are associated with overweight and obese status Arch Intern Med. 2005 165:25-30
The Obesity Epidemic Worldwide Nature 2000
Obesity and the Risk of Heart failure Men NEJM 2002 347:305-13
Goals • Review how disturbed sleep impacts physiology in healthyhumans • Examine the data relating disturbed sleep to morbidity and mortality • Understand how a common sleep disorder (Sleep Apnea) may the contribute to cardiovascular risk • Appreciate the complex interaction between disturbed sleep and physiologic risk in patient populations
Relative Risk of CHD across 10 Years according to Self-Reported Sleep Duration*: Nurses Health Study * N = 76,617 * < 5 > 9 • Covariates: shift work, depression, high cholesterol, diabetes, hypertension, BMI, smoking, snoring, exercise, alcohol consumption, aspirin use, postmenopausal hormone use, family history of MI. Arch Int Med 2003 163:205-209
Impact of Sleep on Survival Sleep Efficiency Sleep Latency Efficiency > 80 % Latency < 30 min Survival Efficiency < 80 % Latency > 30 min Weeks Weeks Psychosomatic Medicine 2003 65:63–73
Stress Brain, Behavior, and Immunity 2003 17: 350–364
Effect of Partial Sleep Deprivation on C-Reactive Protein (n = 5) (n = 4) JACC 2004 43:678–83
Sleep Complaints Heart Failure Patients vs. General Population * * * n = 84 Male (59%) Age = 54.1 + 10.8 NYHA = 2.8 + 0.8 LVEF (%) = 21.7 + 6.3 * * * AACN Clinical Issues 2003 14:477-87 Percentage
Impact of Sleep Difficulties on the Minnesota Living with Heart Failure Questionnaire Aim: To describe self-assessed sleep difficulties, daytime sleepiness, and their relation to HRQOL in men and women with HF, as well as to make a comparison to data from a norm population. Design: Cross-sectional design including 223 patients with HF, New York Heart Association classification II–IV, assessed using the Uppsala Sleep Inventory-Chronic Heart Failure, the Epworth Sleepiness Scale, Medical Outcomes Study 36-Item Short Form Health Survey, and Minnesota Living With Heart Failure Questionnaire. Results: Conclusion: Patients with HF have a reduced HRQOL especially if difficulties maintaining sleep, initiating sleep, and early morning awakenings are involved. J Cardiovasc Nurs 2004 19: 234–242
Goals • Review how disturbed sleep impacts physiology in healthyhumans • Examine the data relating disturbed sleep to morbidity and mortality • Understand how a common sleep disorder (Sleep Apnea) may the contribute to cardiovascular risk • Appreciate the complex interaction between disturbed sleep and physiologic risk in patient populations
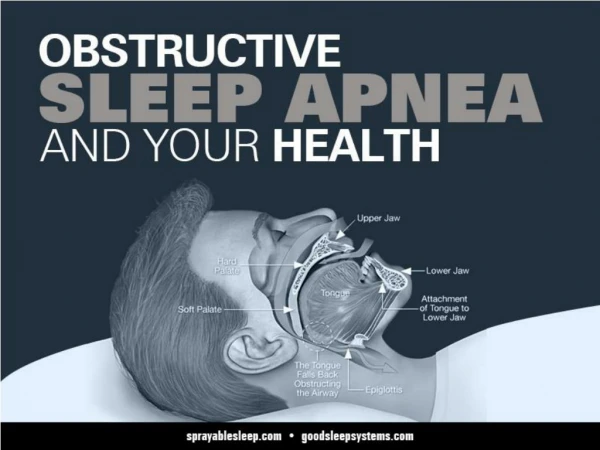
Intermittent Hypoxia Xanthine Oxidase Mitochondrial Dysfunction Homocysteine ROS Activation of Transcription Factors Monocyte Activation Lymphcyte Activation Endothelial cell Activation Adhesion Molecule Expression Monocyte Lymphocyte / Endothelial Adhesion Endothelial Dysfunction Sleep Med Rev 2003 7:35-51 Vascular Disease
OSDB: Effect on Nocturnal BP and CO Thorax 1998 53:416-418
Sympathetic Neural Activity OSA vs. Normals Awake OSA Normal 10 sec J Clin Invest 1995 96:1897-1904
Effect of OSA on Inflammatory Markers IL-6 C-Reactive Protein Circulation 2003 107:1129-34
Effect of Activated Monocytes on the Endothelium Tissue Factor ROS Cytokines MMPs Nature 2002 420: 868-74
Sleep Apnea Impacts on Insulin and Glucose Independent of Obesity J Intern Med 2003 254:32-44
Effect of Long-term Intermittent Hypoxia on Brain Structure and Function • Adult male C57BL/6J mice • 8 week protocol: LTIH during sleep period • Conditions • Sham Intermittent Hypoxia • Intermittent Hypoxia • MSLT performed after 2 weeks of recovery • Basal forebrain and brainstem • Elevated isoprostane (22%) • Increased protein carbonylation 50% • Increased nitration 200% • Induction of antioxidant enzymes Mean Sleep Latency * 12.7 + 0.5 8.9 + 1.0 Sham LTIH (n = 16) LTIH (n =19) Significant oxidative injuries in the sleep-wake regions of the brain after LTIH are associated with “residual hypersomnolence”
Day–Night Pattern of Sudden Death in Obstructive Sleep Apnea Proportion of Sudden Death from all Cardiac Causes (%) Relative Risk of Sudden Death from Cardiac Causes 12:00 – 6:00 AM < 5 > 40 5 -39 10:00 PM – 5:59 AM 6:00 AM – 1:59 PM 2:00 PM – 9:59 PM Apnea Hypopnea Index N Engl J Med 2005 352:1206-14.
Long-term cardiovascular outcomes in men with OSA AIM: Observational study to compare incidence of fatal and non-fatal cardiovascular events in simple snorers, patients with untreated OSA,patients treated with CPAP, and healthy men recruited from the general population. Design: Prospective observational cohort. 264 healthy men, 377 simple snorers, 403 with untreated mild-moderate OSA (AHI 5-30), 235 with untreated severe OSA (AHI > 30), and 372 with OSA and treated with CPAP Cumulative Incidence of Fatal CV Events Cumulative Incidence of Non-fatal CV Events Months Months Conclusion: In men, severe OSA significantly increases the risk of fatal and non-fatal cardiovascular events. CPAP treatment reduces this risk. Lancet 2005 365: 1046–53 .
Goals • Review how disturbed sleep impacts physiology in healthyhumans • Examine the data relating disturbed sleep to morbidity and mortality • Understand how a common sleep disorder (Sleep Apnea) may the contribute to cardiovascular risk • Appreciate the complex interaction between disturbed sleep and physiologic risk in patient populations
Pleiotrophic Effects of Adiopkines on Vascular Risk Obesity Sleep Apnea Diabetes Adipokines & Leptin LV Hypertrophy
Healthy Controls (n = 10) OSA Subjects (n =16) J Appl Physiol 98: 2226–2234, 2005.
Proposed Model Integrating Sleep Disordered Breathing, Psychological Stress and Nocturnal Physiology as Predictors of CVD Risk Factors Sleep SCORE Heart SCORE • Established CV • Risk Factors • Cholesterol • Hyperglycemia • Blood Pressure • Smoking Sleep Disordered Breathing • Cardiovascular • Morbidity & Mortality • Coronary calcification • Brachial artery size • Endothelial dysfunction • MI • Stroke • Death • Nocturnal Physiology • Non SDB sleep Characteristics • Urinary catecholamines • Autonomic function • BP dipping status • Emerging CV • Risk Factors • Inflammation • Metabolic Syndrome • Renal Insufficiency • Psychological stress • Acute & chronic life events • Ambient stress
Sleep and Heart Failure: The role of Autonomic Activation and Inflammation Sleep Drive Wake Drive Sleep Inflammation Sympathetic Activation Heart Failure CRT
Interaction between Sleep and Wake States NREM WAKE REM
Summary • Impaired sleep affects a number of physiologic parameters. • Concomitant primary sleep disorders can “gain up” the stress response. • Understanding the relative contribution of psychological stress vs. metabolic stress is crucial when investigating patient populations. • A collaborative / translational approach is essential to understand mechanisms and advance the field. • Think about sleep when caring for patients and planning research questions.