Download
1 / 32
320 likes | 478 Views
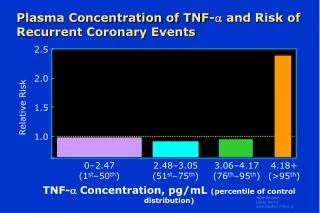
Plasma Concentration of TNF- and Risk of Recurrent Coronary Events. 2.5 2.0 1.5 1.0. Relative Risk. 0–2.47 (1 st –50 th ). 2.48–3.05 (51 st –75 th ). 3.06–4.17 (76 th –95 th ). 4.18+ (>95 th ). TNF- Concentration, pg/mL (percentile of control distribution).

E N D
Plasma Concentration of TNF- and Risk of Recurrent Coronary Events 2.5 2.0 1.5 1.0 Relative Risk 0–2.47(1st–50th) 2.48–3.05(51st–75th) 3.06–4.17(76th–95th) 4.18+(>95th) TNF- Concentration, pg/mL (percentile of control distribution)
Predictive Value of CRP and Other Inflammatory Markers: LDL <130 mg/dL 4 3 2 1 hs-CRP SAA Relative Risk of FutureCoronary Events IL-6 sICAM-1 1 2 3 4 Quartile of Inflammatory Marker
Age-Adjusted Correlation Coefficients for hs-CRP Levels and Lipid Parameters over a 5-Year Follow-up Period
Population Distribution of hs-CRP in Apparently Healthy American Men and Women
Assessment of the Clinical Utility of Novel Markers of Cardiovascular Risk
Is there clinical evidence that inflammation can be modified by preventive therapies?
hs-CRP, Aspirin, and Risks of Future MI: Physicians' Health Study Aspirin Placebo Relative Risk of MI 1 2 3 4 Quartile of C-Reactive Protein
Low-Dose Aspirin Reduces Thromboxane B2 but not CRP 140 120 100 80 60 40 20 0 140 120 100 80 60 40 20 0 28 Days 31 Days Serum CRP (% of Baseline) Serum Thromboxane (% of Baseline) * p<0.001 * * Placebo(n=11) ASA 81 mg qd(n=13) Placebo(n=11) ASA 81 mg qd(n=13)
Reduction of Proinflammatory Cytokines and CRP with Higher-Dose Aspirin in Patients with Chronic Stable Angina
Elevated CRP Levels in Obesity: NHANES 1988-1994 Percent with CRP 0.22 mg/dL Normal Overweight Obese
Effects of Weight Loss on CRPConcentrations in Obese Healthy Women • 83 women (mean BMI 33.8, range 28.2-43.8 kg/m2) placed on very low fat, energy-restricted diet (6.0 MJ, 15% fat) for 12 weeks • Baseline CRP positively associated with BMI (r=0.281, p=0.01) • CRP reduced by 26% (p<0.001) • Average weight loss 7.9 kg, associated with change in CRP • Change in CRP correlated with change in TC (r=0.240, p=0.03) but not changes in LDL-C, HDL-C, or glucose • At 12 weeks, CRP concentration highly correlated with TG (r=0.287, p=0.009), but not with other lipids or glucose
Effects of Weight Loss in Obese Women on IL-6, TNF-, and CRP Before diet After very low calorie diet(mean BMI reduction 2.1 kg/m2; mean reduction in body fat mass 4 kg) p=0.05 p=0.14 p=0.6 mg/L pg/mL IL-6 TNF- CRP
Effects of n-3 Fatty Acid Therapy on Lipids and sCAMs TG TC sICAM-1 sE-selectin * * * Percent Change All Patients * p<0.05 DM Patients *
Effect of HRT on hs-CRP: the PEPI Study 3.0 2.0 1.0 CEE + MPA cyclic CEE + MPA continuous CEE + MP CEE hs-CRP (mg/dL) Placebo 0 12 36 Months
hs-CRP and Relative Risk of Recurrent Coronary Events: CARE P Trend = 0.044 P=0.02 Relative Risk 1<0.12 20.12-0.20 30.21-0.37 40.38-0.66 5>0.66 Quintile of hs-CRP (range, mg/dL)
Inflammation, Pravastatin, and Relative Risk of Recurrent Coronary Events: CARE P Trend = 0.005 Relative Risk Pravastatin Placebo Pravastatin Placebo Inflammation Absent Inflammation Present
Baseline Lipid Levels in Patients with and without Inflammation: CARE 250 200 150 100 50 0 Inflammation absent Inflammation present Mean Baseline (mg/dL) TC LDL-C HDL-C TG
Long-Term Effect of Pravastatin on hs-CRP:CARE Placebo and Pravastatin Groups Placebo 0.25 0.24 0.23 0.22 0.21 0.20 0.19 0.18 –21.6% (P=0.007) Median hs-CRPConcentration (mg/dL) Pravastatin Baseline 5 Years
Change in hs-CRP Concentration Over 5 Years: CARE Subgroup Analyses Placebo Pravastatin All Subjects Age >60 years Age <60 years BMI >27 kg/m2 BMI <27 kg/m2 Smokers Nonsmokers SBP >128 mm Hg SBP <128 mm Hg DBP >78 mm Hg DBP <78 mm Hg LDL-C >138 mg/dL LDL-C <138 mg/dL HDL-C >35 mg/dL HDL-C <35 mg/dL Triglycerides >160 mg/dL Triglycerides <160 mg/dL -0.2 -0.1 0 0.1 0.2 0.3 Change in hs-CRP over 5 Years (mg/dL) Click for larger picture
Change in hs-CRP according to Observed Changes in LDL-C: CARE Placebo and Pravastatin Groups 0.15 Placebo 0.10 Pravastatin 0.05 Change in hs-CRP (mg/dL) 0 -0.05 -0.10 -0.15 Decrease 0–25 Decrease 25–50 Decrease 50–75 Decrease >75 Increase 0–25 Change in LDL-C (mg/dL)
CRP in Combination with LDL-C as a Method to Target Statin Therapy in Primary Prevention: AFCAPS/TexCAPS Event Rate Median LDL-C = 149.1 mg/dLMedian CRP = 0.16 mg/dL
Statin Therapy, Lipid Levels, CRP, and Survival Among Patients with Severe Coronary Artery Disease P Trend <0.0001 P Trend = 0.94 Mortality (%) Medium High Low Medium High Low CRP Tertiles Statins CRP TertilesNo Statins
* * * Effect of Statin Therapy on hs-CRP Levels at 6 Weeks 6 5 4 3 2 1 0 *p<0.025 vs. Baseline hs-CRP (mg/L) Baseline Prava(40 mg/d) Simva(20 mg/d) Atorva(10 mg/d)
12 weeksvs. baseline 24 weeksvs. baseline 24 weeks ITTvs. placebo Effect of Pravastatin on CRP Levels in Primary and Secondary Prevention: PRINCE Primary Prevention Secondary Prevention Change in CRP, % * **p<.005vs. baseline *p<.001vs. baseline ** * ** *
Effect of Bezafibrate with and without Fluvastatin on Plasma Fibrinogen, PAI-1, and CRP in Patients with CAD and Mixed Hyperlipidemia Fibrinogen PAI-1 CRP n: 81 80 74 Change at 24 weeks, % 70 72 63 83 80 75 * P<0.05 vs. baseline * * Beza 400 mg/d+ fluva 20 mg/d Beza 400 mg/d+ fluva 40 mg/d Beza 400 mg/d
CRP in Combination with TC:HDL-C Ratio as a Method to Target Statin Therapy in Primary Prevention: AFCAPS/TexCAPS Event Rate Median TC:HDL-C = 5.96Median CRP = 0.16 mg/dL
Effect of Gemfibrozil and Ciprofibrate on Plasma Fibrinogen and CRP Levels in Patients with Primary Hypercholesterolemia Pretreatment 12 Weeks *p<0.005 vs. pretreatment level * * CRP, mg/L Fibrinogen, g/L Gemfibrozil600 mg bid(n=51) Ciprofibrate100 mg/d(n=48) Gemfibrozil600 mg bid(n=51) Ciprofibrate100 mg/d(n=48)
hs-CRP: Potential Clinical Applications • Adjunct to lipid screening in the detection of individuals at high risk for coronary artery disease • Method to better target statin therapy in the setting of primary prevention • Potential prognostic value in acute coronary syndromes Inflammation is likely to represent a new target for both the treatment and prevention of acute myocardial infarction
Summary • Lifestyle modification and some pharmacotherapies (full-dose ASA, statins) lower hs-CRP • Lipid-modifying therapies with oral estrogens and fibrates are not associated with reduction in hs-CRP • Individuals with high levels of hs-CRP are at increased risk for CHD events and benefit from ASA and statins
Infection and CHD - is there a connection? • Local or systemic infections resulting from gram negative bacteria such as Chlamydia pneumoniae and Helicobacter pylori, including cytomegalovirus (CMV) have been implicated in atheroscelosis • While several case control studies have shown increased titers of C.pneumoniae and H. Pylori in those with vs. without CHD, convincing evidence from prospective studies is lacking.
Prospective Studies of CHD and Infectious Pathogens • Physician’s Health Study (nested case-control) shows RR 1.1 (0.8-1.5) for C. Pneumoniae, 0.94 (0.7-1.2) for cytomegalovirus, and 0.72 (0.6-0.9) for Herpes simplex virus. • H. pylori also shows mixed results. Whincup showed a nonsignificant 1.3 OR when adjusted for other risk factors, the large ARIC study showed no relation, and the Caerphilly Prospective study showed RR=1.05 in 1796 men followed 14 years.
Infectious Agents and the Future • Individuals with greater infectious burdens may be at greater risk, because they are older, have poorer health habits, less access to care. • Observed associations often may be due to selection biases or confounding from age and other factors • Prospective clinical trials under way examining role of certain antibiotics such as azithromycin on reduction of recurrent events in CHD patients. • Until these data are available, no role for measurement or treatment of infectious burden.