Download

1 / 52
680 likes | 2k Views
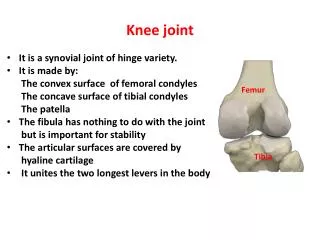
Pathomechanics of Knee Joint. [A]rafat. Screw home “rotation of the knee”. Locking knee on full extension requires knee rotation about 10 degrees .

E N D
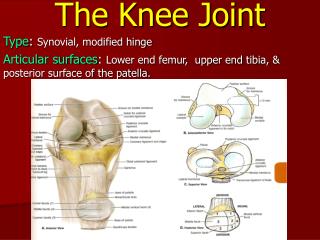
Pathomechanics of Knee Joint [A]rafat
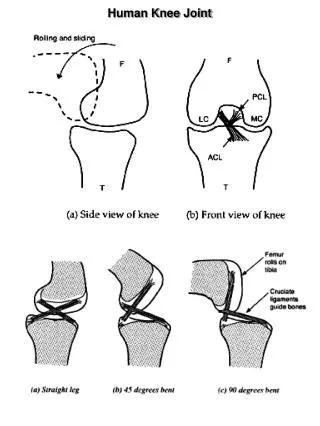
Screw home “rotation of the knee” • Locking knee on full extension requires knee rotation about 10 degrees. • Screw home rotation is different from axial rotation that occur at knee it is a conjunct rotation, linked mechanically to flexion and extension kinematics and cant be performed independently. • Based on observable twisting of knee during last 30 degrees of extension.
In tibio-femoral extension: the tibia externally rotates about 10 degrees. • In femoro-tibialextension (rising from squat): The femur internally rotates on fixed tibia. • Regardless whether tibia or femur is rotating the knee is externally rotated 10 degrees when fully extended.
To observe the screw home mechanism: • at the knee, have the partner sit with the knee flexed to about 90 degrees. • Draw a line on the skin between the tibialtuberosity and the apex of the patella. • After completing full tibial –on femoral extension, redraw this line between the same landmarks and note the change in position of the externally rotated tibia.
Unlocking mechanism • to unlock the knee that is fully extended, the joint must first internally rotate by poplitues muscle that is both internal rotator and flexor of the knee joint, the muscle can rotate femur externally to initiate femoral-on tibial.
flexion, or rotate the tibia internally to initiate tibial –on- femoral flexion. As the extended and locked knee prepares to flex (e.g. when beginning to descend into a squat position), the popliteus provides an internal rotation torque that help mechanically to unlock the knee. In this position the femur is externally rotated on tibia , this action on femur is readily seen by this figure showing line of pull of popliteus
Factors guiding screw home mechanism 1- shape of medial femoral condyle: as it curves 30 degree laterally as it approaches the intercondylar grove. And as and extends further anteriorly than the lateral condyle. Thus tibia must follow this path during tibial on femoral extension. 2- passive tension in the anterior cruciate ligament 3- lateral pull of quadriceps tendon.
Knee joint alignment as in x ray : A) Femoral mechanical axis: centre of femoral head to centre knee.
Knee joint alignment as in x ray : B) Femoral anatomical axis: centre of femoral shaft to center of knee joint. 6o outwards from mechanical axis.
Knee joint alignment as in x ray : C) Tibial mechanical / anatomical axis: centre plateau to centre of talus / ankle.
Assessment of joint alignment using motion analysis: 1- identify bony land marks that marks the beginning and ends of each bony segments (forming the tested joint and marks them by colored markers. 2-Photograph patient in the desired functional position with marks on bony segments ends. 3- Using AutoCAD program draw a straight line that connect between bony segment ends marks. This line represents the mechanical or anatomical axis of the bony segment . 4- Measure the angle between the two drawn anatomical axes.
How to assess knee joint alignment in frontal plane 1- Identify bony land marks: a) Femoral mechanical axis: from centre of femoral head ( 3 fingers medial to ASIS)to centre knee(mid point between medial and lateral femoral epicondyles). Or b) Femoral anatomical axis:centre of femoral shaft (at same level as greater trochanter move anteriorly center of thigh) to centre knee joint (as above). c) Tibial mechanical/anatomical axis (same): from center of knee (mid point between medial and lateral femoral epicondyles) to center of ankle joint (mid point between lateral and medial maleolus.
Normal genuvalgum: normal alignment is distal end of femur makes an angle of 170 -175 with the anatomical axis. • Note: • an angle of 170-175 degree equals • 5-10 degrees valgus
Note that if measuring from mechanical axis the measured angle will increase to the same person, i.e. normal valgus degree is less? Some authors reported that it is 182 degree, i.e. 2 degrees of varus
A) Excessive Genuvalgum(knock knees): the measured angle lateral is less than 165 degree. i.e. genuvalgus degree is >15 degree • Notes: 1- the feet are separated from each others more than knees. 2- the angle opens laterally
B) Genuvarum (bow leg): • the measured angle lateral is more than 185 degree. i.e. genuvarum degree is >5 degree • Notes 1-the feet are nearer to each others than knee. 2-in varus the angle opens medially
How to assess knee joint alignment in sagittal plane 1- Identify bony land marks: Femoral anatomical (mechanical) axis: from greater trochanter to knee to lateral femoral epicondyle. Tibial anatomical (mechanical) axis: from lateral femoral epicondyle to lateral maleoulus. 2-Photograph patient in the anatomical position in sagital view. 3- Using AutoCAD program draw femur and tibia bones axes 4- Measure the front angle between the two drawn axes.
C) Genurecarvatum • the measured angle frontal is more than 190 degree. i.e. genurecarvatum (hyperextension)degree is >10 degree • Notes 1-the knee are leveled beyond the ankle joint
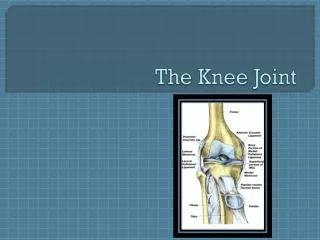
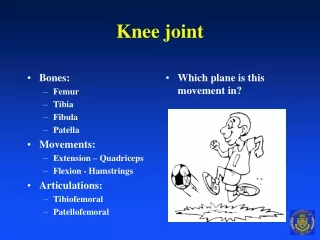
Mensicial Tears • Medial and lateral meniscus are fibro-cartilagenous discs • that deepen the shallow articular surface of tibia • by acting as seats or cushions to femoral condyles. • Medial meniscus is C shaped while lateral meniscus is 0 shaped.
Functions of menisci: 1-Reduce the huge compressive stress at the tibio-femoral joint that may reach 2-3 times body weight during routine knee activity by 230% through trippling the area of joint contact. 2- Stabilizing the joint during motion. 3-Lubricating the articular cartilage. 4-Reducing friction.
Medial meniscus • The medial meniscus is more frequently injured more than lateral meniscus • because its attachment to the medial collateral ligaments. • As medial meniscus movements are more limited than lateral meniscus movements
Common Mechanisms of Mensicial Injury: -Tears of menisci often occurs by forceful horizontal plane rotations of the femoral condyles over a partially weight bearing flexed knee. -A classic complaint of an individual with a mensicial tear (dislodged or flap meniscus) is that the joint locks when he or she attempts to extend the knee from a position of weight bearing, such as rising from a seated position or climbing stairs.
Collateral Ligaments Injury • The medial collateral ligament (MCL): • is a flat, board structure that spans the medial side of the joint. • It resist valgus stress (abduction), extension, and extreme axial rotations.
Common mechanism of injury : • 1-Valgus force with foot planted, • 2- severe hyperextension injury of knee.
b) The lateral (fibular) collateral ligament(LCL): • consists of a round strong cord that runs nearly vertical between the lateral epicondyle and head of fibula. It resist varus stress (adduction), extension, and extreme axial rotations.
Common mechanism of injury : 1-Valgus force with foot planted, 2- severe hyperextension injury of knee.
Cruciate ligaments injury Most of its fibers are taught when knee approaches full extension .
Mechanisms of injury of ACL: 1- Hyperextension of knee. 2- Large valgus force with foot planted on ground. 3-Either of the above combined with large internal axial rotation torque e.g. the femur forcefully externally rotates over a fixed tibia.
Anterior drawer test: • Is based on the fact that ACL provide 85% of passive resistance to anterior translation of tibia, so the test is performed with pulling the tibia forward in knee flexed 90 degrees Anterior translation of 8 mm or 1/3 inch is indicative of a positive ACL injury. It may be masked by hamstring spasm (limiting anterior drawer of tibia).
Relation between muscular contraction and ACL injury: • A contraction of quadriceps muscle extends the knee and slides the tibia anteriorly relative to the femur thus increase the tension in most fibers of the ACL. • While contraction of the hamstring muscle, in contrast. • Causes a posterior translation of the tibia that slackens most fibers of the ACL. • Thus in rehabilitation following injuries over strengthening of hamstrings is an essential component
Functions of (PCL) are: 1- Most fibers resist excessive posterior translation of the tibia or excessive anterior translation of the femur. 2- Most fibers taught in full knee flexion. 3- Some fibers are taught at extremes of varus, valgu and axial rotations
Mechanisms of injury of PCL: 1-Hypeflexion of knee 2- Large valgus or varus force with foot planted . 3- Any of the above, combined with large axial rotation.
Testing PCL injury: • Posterior drawer test: • pushing tibia posteriorly with knee flexed 90 degree • Normally the PCL provide 95% degrees of passive resistance to posterior translation of tibia.
Relation between hamstrings and PCL: • Contraction of hamstrings muscles flexes the knee and slides the tibia posteriorly relative to the femur thus stressing the posterior cruciate ligaments. • A contraction of quadriceps muscle extends the knee and slides the tibia anteriorly relative to the femur thus decreases the tension in most fibers of the PCL. • Thus in rehabilitation following injuries over strengthening of hamstrings is an essential component
Because the cruciate do not spontaneously heal on their on, surgical reconstruction often requires a graft.