Download
1 / 12
130 likes | 238 Views
This systematic review explores the potential benefits of statins in COPD, focusing on their anti-inflammatory effects and impact on various outcomes. The study sources, design, outcomes, and results are discussed, highlighting a range of positive findings in COPD-related outcomes.

E N D
Statins In COPD: A Systematic ReviewSurinder J, Kirly P et al. Chest 2009; 136: 734-743. DivyaBappanad March 11, 2010 Journal Club
Background • COPD is a systemic inflammatory disease not limited to the lung • Increased recruitment and activation of inflammatory cells( neutrophils, eosinophils, lymphocytes and alveolar macrophages) • Increased levels of IL-6, IL-8, CRP, fibrinogen, TNF, and leukocytes • Chronic inflammation persists even after cessation of smoking
Background • Statinspleiotropic anti-inflammatory effects • Decrease neutrophil numbers, T cell activation and differentiation, and increase apoptosis of eosinophils • Also regulate inflammation by increased phagocytosis of apoptotic cells • Murine and rat models demonstrate slowed progression of emphysema with statin use
Methods • Study Sources – Medline, Cochrane, PapersFirst and Excerpta Medical Database as well as bibliographies of found papers • Design of studies included – randomized, single or double blinded, placebo controlled, observational cohort( prospective or restrospective), population based analysis • Study exclusion criteria – laboratory or experimental based studies • Number of studies screened vs. accepted – 264 vs 9 • Outcomes – All cause mortality, COPD related mortality, COPD, the time to and number of COPD exacerbations, the time to an number of COPD intubations, exercise capacity, and pulmonary function FEV1 and FVC
Validity • Focused clinical question addressed • Appropriate study inclusion criteria • No important studies excluded • Significant degree of heterogeneity between studies
Results • 4 retrospective cohort • 1 nested case control of a retrospective cohort • 1 combination retrospective cohort • 2 case control • 1 randominized controlled trial
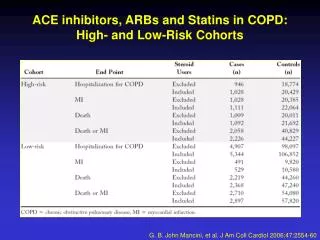
Results • All cause mortality • Mancini et al nested case control • OR 0.53(95% CI 0.43 -0.65) vs OR 0.49(95% CI0.41-0.58) • In both high risk CV and low risk CV group • Soyseth et al retrospective cohort • HR 0.57(95% CI 0.38-0.87) • Van Gestel et al retrospective cohort • short term( 30 day) OR 0.48(95% CI 0.23-1) • long term(10 year) OR (95% CI 0.52-0.86)
Results • COPD related mortality • Frost et al retrospective cohort and case control • Low dose statin OR 0.58(95% CI 0.17-0.92) • Moderate dose statin OR 0.17(95% CI 0.07-0.42) • Dose dependant effect • Ishida et al population based • Annual sales with negative correlation • Correlation coefficient 0.574(p<0.001)
Results • COPD hospitalizations • Keddissi et al retrospective cohort • *0.17+/- 0.31 patients per year vs 0.11 +/-0.26 patients per year • But rate decrease FEV1 and FVC slowed with statin use • Mancini et al • High risk CV OR 0.71(95% CI 0.56 -0.91) • Low risk CV OR 0.71(95% CI 0.64-0.77) • COPD exacerbations • Blamoun et al retrospective cohort • OR 2.35(95% CI 1.01-5.5)
Results • Exercise capacity and CRP • Lee et al RCT • Pravastatin vs placebo • Increased exercise time on treadmill • 599 +/- 323 to 922 +/- 328 s p<0.0001 • Decreased CRP • 3.94 +/- 3.54 to 2.66 +/- 2.49 p<0.0005
Comments • All studies showed benefit in range of COPD related outcomes • Clinical finding correlate to findings in pulmonary systems of animal models • Lack of RCTs mean that confounding variables and bias present • Definitions of COPD varied as did dose and duration of statins
Next steps • Atorvastatin vs placebo for change in peak flow • Simvastatin vs placebo for changes in CRP • Lovastatin vs placebo for changes in apoptosis and efferocytosis in pulmonary macrophages